Radiation optic neuropathy (RON) is an optic nerve disorder caused by delayed ischemic changes following radiation exposure to the optic apparatus. The optic apparatus is highly radiosensitive, and visual function is lost through mechanisms primarily involving vascular endothelial damage.
The most common site is the optic chiasm or its adjacent regions, classified into anterior RON and posterior RON. Anterior RON results from proton beam therapy or plaque brachytherapy for orbital, choroidal, or retinal tumors, while posterior RON arises from treatment of paranasal sinus or skull base tumors.
The risk of onset is closely related to the radiation dose. The following table shows the relationship between dose and risk.
Irradiation Condition
Risk of Onset
Total dose less than 5,000 cGy
Rare
Total dose 5,000–6,000 cGy
Up to 5% within 10 years
Single dose ≤2 Gy, total dose ≤50 Gy
Relatively safe
Gamma Knife 800–1,000 cGy single fraction (1–3 sessions)
Relatively safe
The onset time ranges from 3 months to several years after irradiation, with most cases occurring within 3 years. The peak onset is at 1.5 years after irradiation, and the most common onset is 8–16 months after treatment. With the widespread use of Gamma Knife, the incidence of RON has significantly decreased.
QWhat is the probability of developing radiation optic neuropathy after radiation therapy?
A
With fractionated irradiation at a total dose of less than 5,000 cGy (50 Gy), onset is rare. At 5,000–6,000 cGy, it is reported to occur with a probability of up to 5% within 10 years. A single dose of 2 Gy or less and a total dose of 50 Gy or less are considered relatively safe, and these values serve as standards when planning irradiation.
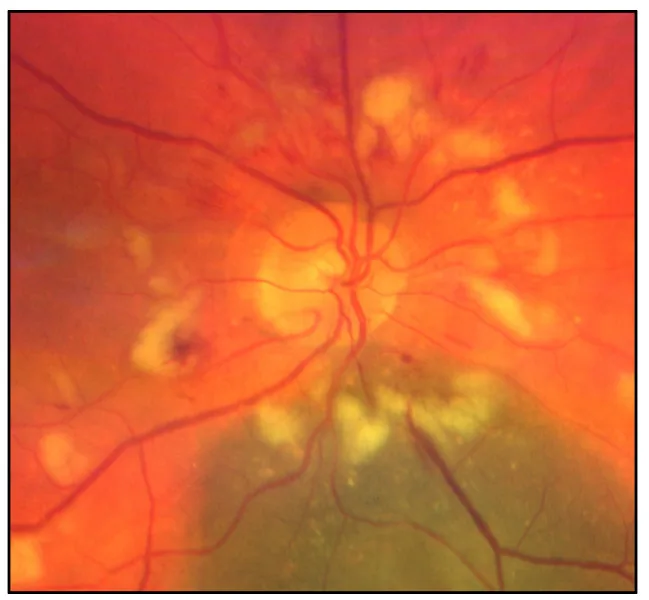
Midena G, et al. Chorioretinal Side Effects of Therapeutic Ocular Irradiation: A Multimodal Imaging Approach. J Clin Med. 2020. Figure 3. PMCID: PMC7693915. License: CC BY.
Color fundus photograph of radiation retinochoroidopathy after laser treatment, showing chorioretinal atrophy, ischemia, ghost vessels, soft exudates, hard exudates, and retinal hemorrhages in both the macula (radiation maculopathy) and the optic nerve (radiation optic neuropathy). This corresponds to radiation optic neuropathy discussed in the section “2. Main Symptoms and Clinical Findings.”
Decreased visual acuity: Presents as progressive and rapid vision loss over several weeks. It can be unilateral or bilateral and is usually painless.
Color vision impairment: Color vision abnormalities are also commonly observed.
Onset pattern: Classified as acute (during treatment), early delayed (3 months after irradiation), and late delayed (6 months to 10 years after irradiation).
If bilateral: Symptoms in the second eye often appear within a few weeks.
A 42-year-old woman (50 Gy irradiation for brain metastasis of breast cancer) presented with superior altitudinal visual field defect, inferior segmental optic disc pallor, and positive RAPD in the right eye one year after irradiation. Eventually, the right eye had only light perception (amaurotic pupil) 1).
A 74-year-old woman (54 Gy irradiation after meningioma resection) had left eye visual acuity of 20/20 and was asymptomatic at 22 months after irradiation, but OCT detected thinning of pRNFL and GCIPL 2).
Radiation damages cells through two pathways: direct disruption of molecular bonds and indirect damage via free radical generation. As stated by the Bergonie-Tribondeau law, cells with high mitotic activity and low differentiation are more susceptible to radiation damage. Damage to vascular endothelial cells leads to increased vascular permeability and capillary occlusion, ultimately causing ischemic optic neuropathy.
Radiation dose: Total dose, dose per fraction, and treatment interval all contribute to risk.
Diabetes: Increases the risk of ischemic vascular disease and elevates the risk of developing RON.
Hypertension and pre-existing vascular lesions: Cases with pre-existing vascular pathology have increased risk.
Concurrent chemotherapy: May potentiate radiation damage.
Patient age: Age is also considered a risk factor.
QDoes having diabetes increase the risk of radiation optic neuropathy?
A
Patients with diabetes have a higher risk of ischemic vascular disease, which is thought to increase the risk of developing RON. Hypertension and pre-existing vascular lesions are also risk factors. Concurrent chemotherapy may further increase the risk. In cases with multiple risk factors, particularly careful radiation planning and follow-up are required.
Giant cell arteritis (differential in elderly patients)
Cerebrospinal fluid analysis via lumbar puncture (to rule out carcinomatous meningitis) and serological tests (to search for paraneoplastic syndromes) may also be necessary.
MRI (first choice): MRI is the first choice for optic nerve diseases, and coronal STIR and Gd-enhanced T1-weighted images are useful. Thin slices of 3T and 3 mm or less are recommended. Contrast enhancement of the affected optic nerve is observed. In the early stage, differentiation from tumor recurrence may be difficult. In the case reported in 2), swelling and contrast enhancement of the left prechiasmatic optic nerve were confirmed on T1 contrast MRI.
OCT: Can detect thinning of pRNFL and GCIPL, and may capture changes before they become symptomatic 2). Its usefulness as a screening tool after radiotherapy has been suggested.
OCT-A (Optical Coherence Tomography Angiography): A grading scale of 0 to 4 based on changes in the radial peripapillary capillary plexus (RPCP) has been proposed, and it is attracting attention as a non-invasive evaluation method.
The following is an overview of the OCT-A grading scale.
Grade
Findings
0
Regular radial distribution of RPCP
1
Loss of initial radial pattern of RPCP
2
Peripapillary hypoperfusion in less than 2 quadrants
3
Hypoperfusion in 2 or more quadrants
4
Diffuse hypoperfusion in all 4 quadrants
Grades 1 to 3 have a ”+” subclass (involvement of the papillomacular bundle), which correlates with decreased visual acuity.
QHow can radiation optic neuropathy be detected early?
A
Detection of pRNFL and GCIPL thinning by OCT may capture changes before subjective symptoms appear 2). MRI shows contrast enhancement of the affected optic nerve. Regular ophthalmic monitoring after radiotherapy is thought to lead to early detection of RON, and some reports propose routine MRI monitoring 10 to 20 months after completion of external beam radiation 2).
There is essentially no curative treatment, and the prognosis is generally poor. For early-stage cases without optic atrophy, the following treatments may be somewhat useful.
Systemic steroid therapy: Administered early in the onset. Cases have been reported with prednisolone 50 mg/day 1). Some cases were treated with prednisone 60 mg/day for 4 weeks 2). However, some reports indicate that steroids and anticoagulation therapy have not been successful for RON.
Anticoagulation therapy: Anticoagulants such as heparin may be used.
Hyperbaric oxygen therapy (HBOT): Performed to promote angiogenesis and inhibit the progression of ischemic necrosis. It is administered as early as possible after symptom onset (within about 72 hours) at 2-3 atmospheres of nearly 100% oxygen for 30-60 minutes. Side effects include barotrauma, bronchopulmonary toxicity, seizures, dry eye, and reversible myopia. It is expensive, and progression may recur after discontinuation.
In 45% of affected eyes, final visual acuity is less than 20/200 to light perception.
Approximately half of cases result in no light perception.
May lead to permanent unilateral or bilateral blindness.
QCan vision be restored with treatment for radiation optic neuropathy?
A
There is no curative treatment, and the prognosis is generally poor. In 45% of affected eyes, final visual acuity is less than 20/200 to light perception, and about half result in no light perception. Systemic steroids, hyperbaric oxygen therapy, and anticoagulation therapy may be somewhat useful for recent-onset cases, but none guarantee recovery of visual function.
The pathogenesis of RON involves both vascular damage (radiation vasculitis) and direct radiation damage to the optic apparatus. Whether the initial damage appears in the vascular system or the neural parenchyma remains unclear.
Reversible inflammation and exudative vascular damage: Increased vascular permeability is central. Changes at this stage are considered reversible.
Progressive stage (months to years)
Vascular occlusion and endothelial cell proliferation: Free radical damage is added.
Microvascular insufficiency: Microvascular insufficiency with hypoxia is induced. Direct damage to cellular DNA and the blood-brain barrier also occurs.
Irreversible stage
Demyelination and reactive astrocytosis: Damage spreads to surrounding nerves, leading to irreversible visual loss.
Radiation-induced cell damage occurs via two pathways. The first is direct damage through disruption of molecular bonds, and the second is indirect damage through free radical generation. According to the Bergonie-Tribondeau law, cells with higher mitotic frequency and less differentiation are more susceptible to damage. Damage to vascular endothelial cells leads to increased capillary permeability and occlusion, and through local VEGF elevation and inflammatory response, ischemic optic neuropathy is established.
7. Latest Research and Future Perspectives (Research-stage Reports)
Bevacizumab has attracted attention as a treatment targeting local VEGF elevation associated with endothelial cell damage. Systemic administration (once every 3 weeks, total of 4 doses) or intravitreal administration (at least 2 doses every 6-8 weeks) has been reported, with reports of stable improvement in visual acuity and color vision over 3 years.
Pentoxifylline (Trental), a methylxanthine derivative, has been shown to modify blood viscosity and may help improve circulation, with promising results reported. In actual case reports, pentoxifylline 1,200 mg/day has been prescribed2).
There is a report that administration of an ACE inhibitor (ramipril) starting 2 weeks after radiation exposure for about 6 months reduces the release of inflammatory cytokines. However, this has only been demonstrated in rat models so far, and its application to humans is not yet established.
Vitamin E has been shown to reduce reactive oxygen species production and inhibit fibrosis in in vitro studies, but clinical evidence is limited.
By detecting thinning of pRNFL and GCIPL on OCT, it may be possible to diagnose radiation optic neuropathy before it becomes symptomatic 2). A grading scale using OCT-A is also expected to be useful as a non-invasive monitoring tool in the future. The establishment of an international registry is expected to further elucidate the clinical profile.
Abduraman S, Maliş B, Celebi ARC.. Taxane-associated retinopathy and radiation-induced optic neuropathy in a young female patient with metastatic breast cancer. GMS Ophthalmol Cases. 2025;15:Doc07. doi:10.3205/oc000255. PMID:40859984; PMCID:PMC12372525.
Grosinger A, Chen JJ, Link MJ, Bhatti MT. Detection of Asymptomatic Radiation Induced Optic Neuropathy with Optical Coherence Tomography. Neuro-ophthalmology (Aeolus Press). 2021;45(5):339-342. doi:10.1080/01658107.2020.1871031. PMID:34566215; PMCID:PMC8409771.