Orbital lymphoma is a general term for lymphoma arising in the ocular adnexa (orbit, lacrimal gland, eyelid, conjunctiva), also called ocular adnexal lymphoma. It accounts for 6–8% of all orbital tumors and 10–15% of ocular adnexal lesions. In Japan, lymphoproliferative disorders are the most common primary orbital tumors, comprising 50–60% of all orbital tumors. Approximately 55% of adult orbital malignancies are lymphoma 6).
Epidemiology and Classification
Incidence: Approximately 1.14 per million per year in the United States 3)
Age of onset: Middle-aged to elderly (60s and older). Diffuse large B-cell lymphoma peaks in the 70s 2)
Sex: Slightly more common in women (reported male-to-female ratio of 1:2.5). Higher frequency in Asian-Pacific populations.
Primary vs Secondary: Primary 73%, secondary 27%3)
Frequency by site: Orbit 43–74%, conjunctiva 20–33%, lacrimal gland 26%, eyelid 9%3)4)
Histological type
The majority are B-cell non-Hodgkin lymphomas (80%), followed by T-cell (14%) and natural killer cell (6%). The most common histological type is mucosa-associated lymphoid tissue lymphoma (70–80% of orbital and conjunctival primary cases, 59% of orbital B-cell lymphomas)5), followed by diffuse large B-cell lymphoma (DLBCL, 8–13%)2), follicular lymphoma, and mantle cell lymphoma.
QIs orbital lymphoma benign or malignant?
A
It is classified as a malignant tumor. However, the degree of malignancy varies greatly depending on the histological type. Mucosa-associated lymphoid tissue lymphoma is low-grade with a good prognosis (5-year survival rate approximately 95%), whereas diffuse large B-cell lymphoma is high-grade, progresses rapidly, and has a poor prognosis.
Decreased vision: Appears when compression of the optic nerve or eyeball progresses.
Foreign body sensation/tearing: Associated with conjunctival lesions or lacrimal duct obstruction.
Mucosa-associated lymphoid tissue lymphoma progresses slowly and painlessly, and eye movement disorders and visual dysfunction are often mild. Diffuse large B-cell lymphoma progresses relatively rapidly, and may develop within one month 2). B symptoms (fever, night sweats, weight loss) appear in about one-third of patients 2).
Asroui L, Hamam RN. Classification, diagnosis, and management of conjunctival lymphoma. Eye Vis (Lond). 2019;6:22. Figure 1. PMCID: PMC6660942. License: CC BY 4.0.
Slit-lamp photograph showing a salmon patch (salmon-colored soft submucosal mass) in the superotemporal conjunctiva of the right eye; lymphoma was confirmed by biopsy. This corresponds to the characteristic conjunctival finding of MALT lymphoma discussed in the section “2. Main Symptoms and Clinical Findings.”
Slow progression: Painless, enlarging over months to years.
Molding pattern: A homogeneous mass that fills the spaces between the globe, extraocular muscles, and optic nerve like a cast. Borders are relatively well-defined.
Salmon-pink mass: Lesions arising in the conjunctiva present as a soft, salmon-colored mass (salmon patch).
Lacrimal gland involvement: S-shaped eyelid deformity and a firm palpable mass.
Bilaterality: Seen in 25% of cases 1).
High-grade (e.g., diffuse large B-cell lymphoma)
Rapid progression: Accompanied by inflammatory signs, with acute proptosis developing over weeks.
Proptosis: Measured with an exophthalmometer (Hertel method). Marked in high-grade types 4) (proptosis in 54% 4)).
Corneal complications: Marked proptosis can lead to corneal exposure and perforation 2).
QWhat symptoms often lead to the discovery of orbital lymphoma?
A
Painless mass (67%) and proptosis (54%) are the most common 4). Many cases are asymptomatic and slowly progressive, so they are sometimes discovered incidentally during cosmetic surgery 3). When ocular motility restriction (39%) is added, diplopia may be reported.
The “infection-inflammation-mutation (IMM) model” has been proposed for the development of orbital lymphoma. In this model, chronic antigenic stimulation leads to persistent proliferation of lymphoid tissue, eventually resulting in malignant transformation.
Infection/Pathogens
Chlamydia psittaci: Association with mucosa-associated lymphoid tissue lymphoma has been reported 5)
Helicobacter pylori, human herpesvirus, HIV, Toxoplasma gondii: Involvement is suggested but controversial
Immunodeficiency: Aging, HIV/AIDS, and immunosuppressive drugs causing immune suppression 6)
Autoimmunity/Inflammation
Sjögren’s syndrome and other autoimmune diseases are associated 5)
Chronic inflammatory orbital disease: Some cases are diagnosed as lymphoma after long-term steroid treatment 8)
Abnormal activation of the NF-κB pathway (mediated by GNL3L) promotes B-cell proliferation 5)
Genetic polymorphisms of TNF and IL-10 are involved in the development of diffuse large B-cell lymphoma
Histological transformation from MALT type to diffuse large B-cell lymphoma: Occurs in more than 8% of MALT lymphomas 7)
QIs there a way to prevent orbital lymphoma?
A
No specific preventive method has been established. The development involves multiple factors such as infection, chronic inflammation, and genetic mutations, and no single risk factor has been identified.
Definitive diagnosis cannot be made based solely on clinical and imaging findings; incisional biopsy (open biopsy) is essential. The biopsy specimen is divided and processed for the following purposes:
Formalin fixation: for routine histopathological examination
Cell culture medium (e.g., RPMI): for flow cytometry
Cryopreservation: for genetic testing (PCR, Southern blot)
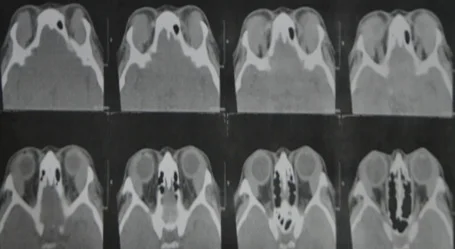
Wabwire D, Nkanga D, Nzunza R, et al. Atypical lymphoid proliferation of the orbit. Open Ophthalmol J. 2022;16:e187436502209260. Figure 3. PMCID: PMC8900200. License: CC BY 4.0.
Axial non-contrast CT shows homogeneous soft tissue masses in both orbits surrounding the globes and extraocular muscles like a mold, without bone destruction. This corresponds to the molding pattern (typical CT finding of orbital lymphoma) discussed in section “4. Diagnosis and Examination Methods”.
CT: Typical appearance is a homogeneous mass that conforms to surrounding structures without bone destruction. High-grade tumors may show bone destruction and heterogeneous mass.
MRI: Iso- to hypointense on T1-weighted images, iso- to hyperintense on T2-weighted images, homogeneous contrast enhancement. MRI is excellent for evaluating molding patterns. Recommended sequences are T2-weighted STIR and T1-weighted gadolinium-enhanced with fat suppression. Malignant lymphoma tends to have more distinct borders compared to idiopathic orbital inflammation.
QCan orbital lymphoma be diagnosed by imaging alone?
A
No. CT and MRI are useful for evaluating molding patterns and homogeneity of the mass, but incisional biopsy is essential for definitive diagnosis. Imaging findings are only grounds for suspicion, and treatment should not be initiated without histopathological diagnosis.
Treatment strategy is determined by a combination of histopathological grade and clinical stage. For high-grade lymphoma or systemic disease, referral to a hematologist-oncologist is essential.
Indications: Elderly patients for whom R-CHOP is unsuitable.
Regimen: Rituximab 375 mg/m² plus bendamustine 90 mg/m² (day 2), every 28 days. Good efficacy and tolerability have been reported in elderly patients7).
Rituximab (anti-CD20 monoclonal antibody): damages tumor cells through three mechanisms: induction of apoptosis, complement-mediated cell lysis, and antibody-dependent cellular cytotoxicity2)
There are reports of efficacy as monotherapy in secondary orbital lymphoma (chronic lymphocytic leukemia/small lymphocytic lymphoma, etc.)3)
The main purpose is biopsy for definitive diagnosis. Total resection carries a risk of damaging important orbital structures and is usually not indicated.
Radiotherapy 30 Gy (observation is also an option)
Low grade
Systemic disease (Stage III or higher)
CHOP therapy or R-CHOP therapy
High-grade (diffuse large B-cell lymphoma, etc.)
All stages
Chemotherapy (R-CHOP, etc.) ± radiation
QCan vision be preserved with treatment for orbital lymphoma?
A
For localized MALT lymphoma, radiation therapy achieves a local control rate of over 90%, and visual function can be preserved in most cases 5). However, doses exceeding 30 Gy increase the risk of complications such as radiation cataract. In high-grade lymphomas like diffuse large B-cell lymphoma, rapid tumor progression and corneal damage due to proptosis may threaten vision 2).
A three-step model of infection → inflammation → mutation (IMM model) has been proposed for the development of ocular adnexal lymphoma. Chronic antigenic stimulation leads to persistent proliferation of lymphoid tissue, eventually accumulating genetic mutations and undergoing malignant transformation.
The cell of origin for major histological types is as follows:
MALT lymphoma (extranodal marginal zone lymphoma): derived from memory B cells of mucosa-associated lymphoid tissue
Follicular lymphoma: derived from germinal center B cells
Mantle cell lymphoma: derived from naive B cells of the mantle zone
Transformation to diffuse large B-cell lymphoma occurs in more than 8% of MALT lymphomas 7). Conversion to large tumor cells is observed in areas with a high Ki67 proliferation index. Prognosis worsens significantly after transformation; therefore, biopsy for tissue confirmation is necessary when exacerbation or rapid progression is noted during follow-up.
Low-dose radiation therapy (2 Gy × 2 fractions = 4 Gy) for slowly progressive ocular adnexal lymphoma is being investigated as an alternative to moderate-dose radiation therapy. It is expected to reduce the risk of complications, but further study is needed on local control rates.
For Chlamydia psittaci-associated mucosa-associated lymphoid tissue lymphoma, tumor regression with antibiotics (e.g., doxycycline) has been reported. However, the involvement of Chlamydia psittaci varies geographically, so the effect differs greatly by region5).
Wang et al. (2026) reported the NF-κB pathway (GNL3L-mediated), IL-27RA pathway, and p53 pathway as new therapeutic targets in the pathogenesis of mucosa-associated lymphoid tissue lymphoma5). Metabolic reprogramming (enhanced glycolysis and lipid synthesis) is also attracting attention as a novel therapeutic target contributing to immune resistance.
Sharif MW, Mungara S, Bajaj K, et al. Orbital lymphoma masquerading as euthyroid orbitopathy. Cureus. 2023;15(2):e34885.
Balasubaramaniam D, Singh S, A Qamarruddin F, et al. Bilateral large orbital lymphoma with proptosis. Cureus. 2023;15(3):e36548.
Anderson DL, Gruizinga BA, Dean HC, et al. Incidental diagnosis of four lid orbital lymphoma during a blepharoplasty. Plast Reconstr Surg Glob Open. 2024;12:e5870.
Urrutia YA, Fezza T, Kosek K, et al. Case series of orbital lymphoma: cardinal presentations. Plast Reconstr Surg Glob Open. 2024;12:e5913.
Wang YF, Chen HC, Lin FC, et al. Atypical orbital mucosa-associated lymphoid tissue lymphoma involving the inferior rectus in a young adult: a case report and literature review. Medicine. 2026;105(4):e47240.
Chaurasiya BD, Agrawal G, Chaudhary S, et al. Orbital lymphoma masquerading as orbital cellulitis. Case Rep Ophthalmol Med. 2021;2021:8832783.
Huang CH, Kung WH, Chang CH, et al. Bilateral lacrimal glands and paranasal sinus diffuse large B-cell lymphoma following lung mucosa-associated lymphoid tissue lymphoma in one patient. Taiwan J Ophthalmol. 2022;12:101-105.
Tahri S, Alaoui H, Bachir H, et al. Chronic inflammatory orbitopathy hiding orbital lymphoma. Cureus. 2022;14(3):e23040.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.