Thyroid eye disease (TED) is an autoimmune disease in which immune dysfunction associated with thyroid abnormalities induces inflammation of orbital tissues, increasing the volume of orbital fat and extraocular muscles. Increased retrobulbar tissue pressure leads to proptosis. It most commonly occurs with hyperthyroidism (Graves’ disease), but can also develop as euthyroid ophthalmopathy with normal thyroid function. Thyroid eye disease progresses independently of thyroid hormone levels and is one of the autoimmune diseases involving thyroid-related autoantibodies.
Approximately 40–50% of patients with Graves’ disease develop ocular symptoms. Severe orbital involvement is relatively rare, occurring in 5–10% of all Graves’ disease patients.
The prevalence is reported as 16/100,000 person-years in women and 2.9/100,000 person-years in men1). The age of onset has a bimodal peak in the 40s-50s and 60s-70s1). Smoking is the greatest risk factor for thyroid eye disease and significantly increases the risk of onset2). Younger patients typically present with proptosis as the main feature, while older patients present with diplopia as the main feature, showing an age-related pattern.
The natural course of thyroid eye disease follows the Rundle curve, transitioning from an active (inflammatory) phase, usually lasting 1-3 years, to a stable (non-inflammatory) phase3). The timing of treatment intervention is determined based on this curve.
Upper eyelid swelling, upper eyelid retraction, and upper eyelid lag are characteristic.
Dalrymple sign: Widening of the palpebral fissure due to upper eyelid retraction.
von Graefe sign: Lid lag (delayed descent of the upper eyelid on downward gaze).
Proptosis
More common in young people (due to fragility of orbital supporting tissues).
Assessed with the Hertel exophthalmometer. Normal range in Japanese individuals is 10–15 mm (mean 13 mm). A difference of ≤2 mm between eyes is normal.
Diplopia
More common in elderly people. Caused by restrictive strabismus due to inflammation and fibrosis of the extraocular muscles.
The inferior rectus is most frequently affected → upward gaze limitation is the most common. Next is abduction limitation due to medial rectus involvement.
DON occurs in about 5% of all cases1) and requires urgent intervention. Signs include positive RAPD, decreased CFF, and visual field defects.
QCan thyroid eye disease develop even if thyroid hormone levels are normal?
A
It can occur as euthyroid ophthalmopathy even when thyroid function is normal. Thyroid eye disease is an autoimmune disease that progresses independently of thyroid hormone levels, and can develop if thyroid-related autoantibodies (TRAb, TSAb) are positive. If eyelid retraction or proptosis is present, testing for thyroid-related autoantibodies is necessary even if thyroid function is normal.
In the early stage, dryness, irritation, tearing, and photophobia are predominant. As the condition progresses, periorbital swelling, proptosis, diplopia, and eyelid retraction become apparent, and in severe cases, corneal ulceration and compressive optic neuropathy may occur.
The following eyelid findings are characteristic of thyroid eye disease.
Sign Name
English Name
Finding
Dalrymple sign
Dalrymple sign
Widening of the palpebral fissure due to upper eyelid retraction, exposing the sclera above the superior corneal limbus.
von Graefe sign
Lid lag
Delayed descent of the upper eyelid on downward gaze.
Stellwag sign
Stellwag sign
Decreased blinking and incomplete eyelid closure
Gifford sign
Gifford sign
Difficulty in everting the upper eyelid
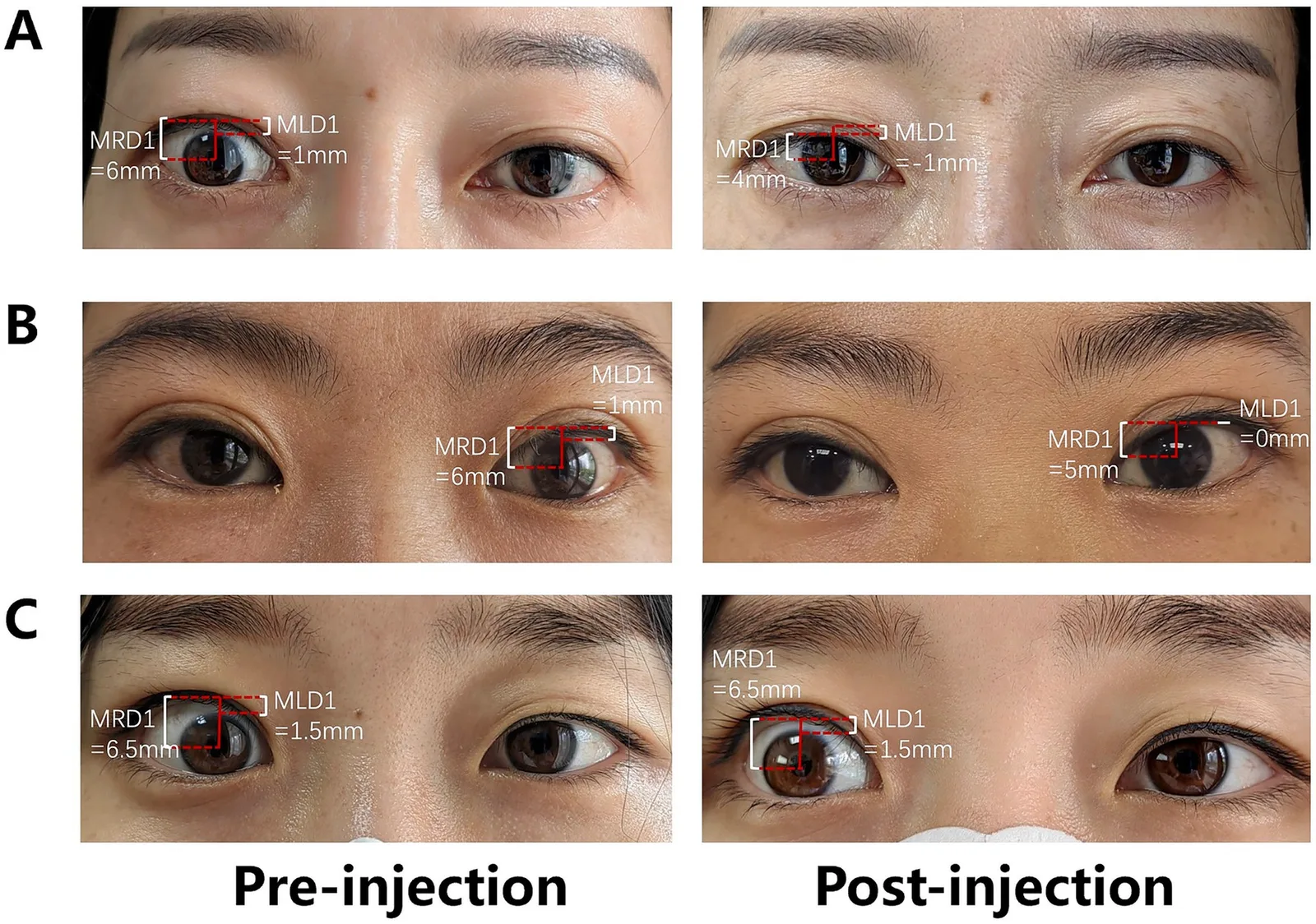
Wang M, Luan Y, Qian Z, Wang Y, Fang W. Percutaneous para-levator palpebrae superioris and subconjunctival injection of triamcinolone acetonide for upper eyelid retraction in thyroid-associated ophthalmopathy. Front Med (Lausanne). 2025;12:1679057. Figure 2. DOI: 10.3389/fmed.2025.1679057. PMCID: PMC12457333. License: CC BY.
In the pre-injection images, MRD1 is enlarged to 6-6.5 mm and scleral show is visible above the superior corneal limbus. This image helps illustrate Dalrymple sign, in which the palpebral fissure is widened in primary gaze.
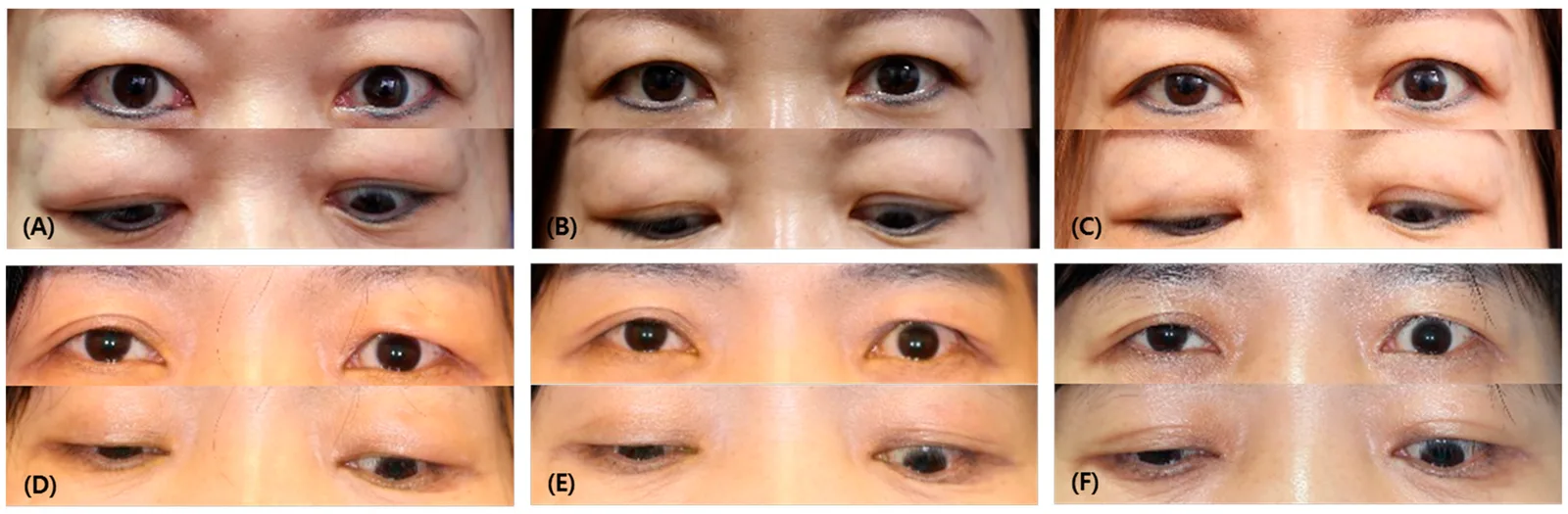
Kim Y, Lew H. Synergistic Therapy for Graves’ Ophthalmopathy-Associated Eyelid Retraction: Steroid, 5-FU, and Botulinum Neurotoxin a Combination. J Clin Med. 2024;13(10):3012. Figure 1. DOI: 10.3390/jcm13103012. PMCID: PMC11121829. License: CC BY 4.0.
These photographs include primary gaze and downgaze views in patients with upper eyelid retraction and help illustrate lid lag, in which the upper eyelid remains relatively high on downgaze. von Graefe sign is a dynamic finding observed as gaze moves from up to down; it should not be diagnosed from a still image alone.
Proptosis is measured using the Hertel exophthalmometer. The normal range in Japanese individuals is 10–15 mm (mean 13 mm), and a difference of 2 mm or less between eyes is considered normal. A Hertel value greater than 18 mm suggests proptosis1).
This occurs when thickened extraocular muscles compress the optic nerve at the orbital apex. It develops in approximately 5% of all cases 1) and is highly urgent. Positive RAPD (relative afferent pupillary defect), decreased CFF (critical flicker frequency), and visual field defects are early signs. Color vision abnormalities are also important findings.
Pain, diplopia, and changes in appearance are the main factors reducing quality of life. The comorbidity rate of anxiety and depression in patients with thyroid eye disease is 36%, approximately twice that of the general population (18.9%) 5). 62% of patients with moderate disease and 89% of those with severe disease have high QOL impairment (score ≥4/7 points) 5). QOL reduction comparable to or worse than that of diabetes, emphysema, and heart failure has been reported.
QWhy does double vision occur in thyroid eye disease?
A
It is caused by restrictive strabismus due to inflammation and fibrosis of the extraocular muscles (especially the inferior rectus), leading to hypertrophy and contracture that restrict normal eye movement. The inferior rectus is most frequently affected, resulting in limited upward gaze. The order of extraocular muscle involvement is inferior rectus > medial rectus > superior rectus > lateral rectus, and it is more common in older adults.
Immune dysfunction associated with thyroid abnormalities triggers inflammation in orbital tissues. Autoantibodies (TRAb) against the TSH receptor (TSHR) activate TSHR on orbital fibroblasts, leading to production of inflammatory cytokines (TNF-α, IL-6, IL-1β, etc.). CD4+/CD8+ T cells infiltrate orbital tissues and amplify the inflammatory response.
Activated fibroblasts increase synthesis of glycosaminoglycans (GAG) and hyaluronic acid, causing tissue edema and water retention. Differentiation of fibroblasts into adipocytes and myofibroblasts leads to expansion of orbital fat and fibrosis of extraocular muscles3).
The IGF-1 receptor (IGF-1R) forms a complex with TSHR and synergistically participates in the activation of orbital fibroblasts 4). This mechanism is the therapeutic target of teprotumumab (IGF-1R inhibitor).
Smoking is the greatest risk factor, associated with disease onset, severity, and treatment resistance 2). Other factors include unstable thyroid function, the acute phase after radioactive iodine therapy, and older age and male sex, which contribute to the risk of severe disease.
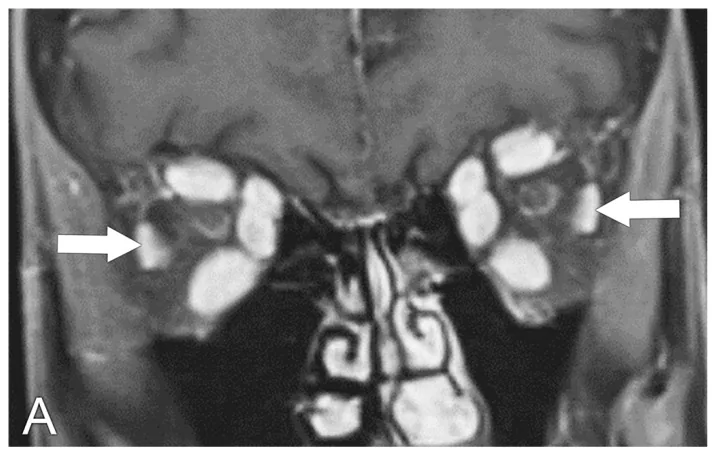
Hutchings KR, Fritzhand SJ, Esmaeli B, et al. Graves’ Eye Disease: Clinical and Radiological Diagnosis. Biomedicines. 2023;11(2):312. Figure 2A. PMCID: PMC9953404. License: CC BY 4.0.
Coronal T1-weighted contrast-enhanced MRI shows marked hypertrophy of the extraocular muscles (arrows) in both orbits, with relative sparing of the lateral rectus, demonstrating the characteristic asymmetric muscle belly enlargement pattern of TED. This corresponds to the extraocular muscle thickening (tendon sparing, muscle belly enlargement) discussed in the section “4. Diagnosis and Examination Methods.”
The triad of eyelid retraction, proptosis, and diplopia strongly suggests TED clinically. Even if thyroid function is normal, positive thyroid-related autoantibodies can lead to a diagnosis of TED.
Measure thyroid hormones (FT₄, FT₃), TSH, and thyroid autoantibodies. Targets include TRAb (TSH receptor antibody), TSAb (thyroid-stimulating antibody), anti-TG antibody (anti-thyroglobulin antibody), and anti-TPO antibody (anti-thyroid peroxidase antibody). At least one of these will be positive.
MRI (first choice): T1-weighted images assess extraocular muscle morphology. STIR (short-TI inversion recovery) sequences show inflamed areas as high-signal regions, useful for evaluating inflammatory activity. Coronal views are essential as they allow simultaneous assessment of all extraocular muscles except the inferior oblique. Axial views evaluate the medial and lateral rectus muscles.
CT: Extraocular muscle thickening (a pattern where the tendon is spared and the belly is enlarged, characteristic of TED) is confirmed, and bone windows are used to evaluate the orbital bone walls.
B-scan ultrasound: Used adjunctively to evaluate extraocular muscle hypertrophy.
The classification according to the 2021 clinical practice guidelines of EUGOGO (European Group on Graves’ Orbitopathy) 1). The NOSPECS classification (classes 0–6) and the VISA classification (Vision, Inflammation, Strabismus, Appearance) are also used for severity assessment.
It is a 7-item scoring system (0–7 points) that evaluates the inflammatory activity of thyroid eye disease. The seven items assessed are: ① spontaneous retrobulbar pain, ② pain on eye movement, ③ eyelid redness, ④ eyelid swelling, ⑤ conjunctival redness, ⑥ conjunctival edema, and ⑦ caruncle/plica swelling. A score of 3 or more indicates the active phase. It is an important indicator for treatment selection and is used to determine the indication for steroid pulse therapy or teprotumumab.
Normalization of thyroid function is essential, and collaboration with an endocrinology department is indispensable. Smoking cessation guidance is implemented in all cases to eliminate smoking, which is the greatest risk factor for disease exacerbation and treatment resistance.
Selenium supplementation: For mild TED, selenium 200 μg/day for 6 months is beneficial and recommended for improving disease activity10).
Corneal and ocular surface protection: Frequent use of artificial tears and corneal protective eye drops, and application of eye ointment before sleep are basic measures. For severe lagophthalmos, consider lateral tarsorrhaphy.
5-2. Steroid therapy (standard treatment for active phase)
Steroid pulse therapy (first-line): Administer methylprednisolone 500–1,000 mg/week for 6–12 weeks1). Intravenous steroids are more effective than oral steroids9). A cumulative dose of ≤8 g is recommended (to reduce risk of liver damage).
Standard protocol: Administer methylprednisolone 1 g × 3 days as one course.
Oral prednisolone: For moderate to severe cases where intravenous administration is difficult, start at 1 mg/kg/day.
Local steroid injection: For upper eyelid edema and inflammatory eyelid retraction, local injection of triamcinolone acetonide (Kenacort-A® 1 ampule) is effective.
Teprotumumab (IGF-1R inhibitor): This is a treatment expected to improve proptosis and diplopia in active moderate-to-severe TED. A meta-analysis of 5 RCTs (total 411 patients) confirmed a significant reduction in proptosis, a significant improvement in the achievement rate of CAS 0–1 at 24 weeks, and a significant improvement in diplopia improvement rate 4), with no significant increase in serious adverse events. Evidence has been established in two major RCTs: Smith et al. (2017, 42 vs 45 patients) 7) and Douglas et al. (2020, 41 vs 42 patients) 8).
Rituximab (anti-CD20 monoclonal antibody): A multicenter randomized trial has shown that it may reduce disease activity in refractory moderate-to-severe TED 12).
Tocilizumab (IL-6 receptor inhibitor): Its use is being considered for cases refractory to steroids and rituximab.
For moderate-to-severe TED, it is administered in combination with immunosuppressive therapy. Typically, 20 Gy in 10 fractions is delivered over 2 weeks. Combination with steroids is considered more effective than monotherapy.
Surgery is generally planned after entering the stable phase of the Rundle curve and when inflammation has subsided. The order of procedures must be strictly followed, as the outcome of the preceding surgery directly affects the subsequent surgical plan.
Surgical techniques and effects: There are five types of procedures combining medial wall, floor, lateral wall, and fat. One-wall decompression achieves -1.4 to -2.3 mm reduction in proptosis, while three-wall plus fat decompression achieves -4.6 to -5.0 mm reduction.
A multicenter study of 633 eyes confirmed stable reproducibility without significant differences among surgeons using the same technique11).
Step 2: Strabismus Surgery
Indications: Diplopia and ocular motility disorders after stabilization of the non-inflammatory phase
Basic procedure: Inferior rectus recession is the most common procedure. The amount of surgery is determined according to the degree of restrictive strabismus.
Indications: Eyelid retraction, functional and cosmetic problems in the stable non-inflammatory phase
Surgical procedure: For upper eyelid retraction, Müller muscle resection or levator recession is selected. Good outcomes have been reported with a combination of Müller muscle resection and levator recession.
QIn what order are surgeries for thyroid eye disease performed?
A
Orbital decompression → strabismus surgery → eyelid surgery, in that order. It is important to follow this sequence because the results of the preceding surgery affect the planning of subsequent surgeries. In principle, all surgeries are planned after entering the inactive phase (stable phase of the Rundle curve). Performing surgery during the active phase increases the risk of postoperative fluctuations and recurrence.
QWhat kind of drug is teprotumumab?
A
It is a monoclonal antibody that inhibits the IGF-1 receptor (IGF-1R). It blocks the complex signaling of IGF-1R and TSHR on orbital fibroblasts, suppressing inflammation and tissue expansion. A meta-analysis of five RCTs (total 411 patients) confirmed significant improvements in proptosis, diplopia, and CAS. There is no significant increase in serious adverse events, but long-term safety (hearing impairment, hyperglycemia, etc.) is still being evaluated.
Immune dysfunction associated with thyroid dysfunction induces inflammation of orbital tissues, increasing the volume of orbital fat and extraocular muscles. Elevated retrobulbar tissue pressure causes proptosis.
Pathology of orbital fat: Adipocyte enlargement and lymphocytic infiltration of the interstitium occur, with edema and scar formation due to chronic inflammation. Increased synthesis of glycosaminoglycans (GAG) and hyaluronic acid leads to fluid retention and swelling of the tissue.
Pathology of extraocular muscles: Lymphocyte-predominant inflammatory cell infiltration is seen between striated muscle fibers, causing degeneration and necrosis of muscle fibers. Interstitial edema and thickening due to inflammation occur, and connective tissue proliferates between muscle fibers, leading to extraocular muscle hypertrophy. The inferior rectus is most frequently affected, followed by the medial rectus, superior rectus, and lateral rectus in decreasing order. Therefore, upward gaze impairment is most common, followed by abduction impairment.
① Pathology of the levator palpebrae superioris muscle: Inflammation causes edema of muscle cells, leading to eyelid edema. Adipose tissue infiltrates between muscle fibers, and muscle cells undergo necrosis and scarring, altering levator function.
②Pathology of Müller’s muscle: Müller’s muscle, a smooth muscle under sympathetic innervation, undergoes sustained contraction due to sympathetic hyperactivity associated with hyperthyroidism, elevating the tarsal plate and widening the palpebral fissure.
Autoantibodies against the TSH receptor (TRAb) activate TSHR on orbital fibroblasts, producing inflammatory cytokines (TNF-α, IL-6, IL-1β) via downstream signaling. CD4+/CD8+ T cells infiltrate orbital tissues and amplify the inflammatory response. Activated fibroblasts differentiate into adipocytes and myofibroblasts, causing orbital fat expansion and extraocular muscle fibrosis, respectively3).
IGF-1R forms a complex with TSHR and synergistically participates in the activation of orbital fibroblasts4). Blockade of this complex signaling is the mechanism of action of teprotumumab.
The natural course from the active inflammatory phase (usually 1–3 years) to the stable (non-inflammatory) phase has been conceptualized as the Rundle curve13). Actual treatment interventions are selected after assessing activity and severity1). Anti-inflammatory treatment is prioritized during the active phase, and surgical planning is performed during the non-inflammatory stable phase.
Data continues to accumulate even after FDA approval. A meta-analysis of 5 RCTs (total 411 cases)4) has confirmed efficacy and safety, but results from Phase IV trials are awaited for long-term safety (long-term outcomes such as hearing impairment and hyperglycemia). The possibility of expanding the indication to inactive TED is also being considered.
Improved Accuracy of Orbital Decompression Surgery
A multicenter study involving 7 facilities, 7 surgeons, and 633 eyes 11) confirmed that when the same surgical procedure was performed, there was no significant difference between surgeons. This is an important finding supporting the statistical validity of multicenter RCTs. Endoscopic medial wall decompression has been reported to achieve significantly greater proptosis reduction (-3.67mm vs -2.97mm, p=0.008) compared to open surgery for medial wall plus floor decompression. It has also been shown that preoperative proptosis is significantly associated with postoperative change in proptosis (p<0.001), reaffirming the importance of preoperative assessment.
Fluctuations in TRAb and TSAb during the active phase are correlated with CAS, and research on treatment selection based on biomarkers is ongoing. Large-scale RCTs of tocilizumab (IL-6 inhibitor) for refractory cases are awaited.
Bartalena L, Kahaly GJ, Baldeschi L, et al. The 2021 European Group on Graves’ orbitopathy (EUGOGO) clinical practice guidelines for the medical management of Graves’ orbitopathy. Eur J Endocrinol. 2021;185(4):G43-G67. doi:10.1530/EJE-21-0479. PMID:34297684.
Mark F. Prummel. Smoking and Risk of Graves’ Disease. JAMA. 1993;269(4):479. doi:10.1001/jama.1993.03500040045034.
Bahn RS. Graves’ ophthalmopathy. N Engl J Med. 2010;362(8):726-738.
Cong X, Pei L, Hu H. Teprotumumab for treating active thyroid eye disease: a meta-analysis. Medicine. 2024;103(18):e38059.
Wang Y, Sharma A, Padnick-Silver L, Francis-Sedlak M, Holt RJ, Foley C, et al. Physician-Perceived Impact of Thyroid Eye Disease on Patient Quality of Life in the United States. Ophthalmology and therapy. 2021;10(1):75-87. doi:10.1007/s40123-020-00318-x. PMID:33196932; PMCID:PMC7886952.
Mourits MP, Koornneef L, Wiersinga WM, Prummel MF, Berghout A, van der Gaag R. Clinical criteria for the assessment of disease activity in Graves’ ophthalmopathy: a novel approach. The British journal of ophthalmology. 1989;73(8):639-44. doi:10.1136/bjo.73.8.639. PMID:2765444; PMCID:PMC1041835.
Smith TJ, Kahaly GJ, Ezra DG, et al. Teprotumumab for thyroid-associated ophthalmopathy. N Engl J Med. 2017;376(18):1748-1761. doi:10.1056/nejmoa1614949.
Douglas RS, Kahaly GJ, Patel A, et al. Teprotumumab for the treatment of active thyroid eye disease. N Engl J Med. 2020;382(4):341-352. doi:10.1056/nejmoa1910434.
Kahaly GJ, Pitz S, Hommel G, Dittmar M. Randomized, single blind trial of intravenous versus oral steroid monotherapy in Graves’ orbitopathy. The Journal of clinical endocrinology and metabolism. 2005;90(9):5234-40. doi:10.1210/jc.2005-0148. PMID:15998777.
Marcocci C, Kahaly GJ, Krassas GE, Bartalena L, Prummel M, Stahl M, et al.; European Group on Graves’ Orbitopathy. Selenium and the course of mild Graves’ orbitopathy. N Engl J Med. 2011;364(20):1920-1931. PMID: 21591944. doi:10.1056/NEJMoa1012985.
Hong A, Shoji MK, Villatoro GA, et al. Intersurgeon variability in proptosis reduction after orbital decompression for thyroid eye disease: a multicenter analysis. Ophthalmic Plast Reconstr Surg. 2024;40(3). doi:10.1097/iop.0000000000003090.
Salvi M, Vannucchi G, Campi I, et al. Rituximab treatment in active moderate-to-severe Graves’ orbitopathy: an international, multicenter, single-blind, randomized placebo-controlled study. J Clin Endocrinol Metab. 2015;100(11):422-431.
Rundle FF, Wilson CW. Development and course of exophthalmos and ophthalmoplegia in Graves’ disease with special reference to the effect of thyroidectomy. Clin Sci. 1945;5(3-4):177-194. PMID: 21011937.