Scleral Exposure
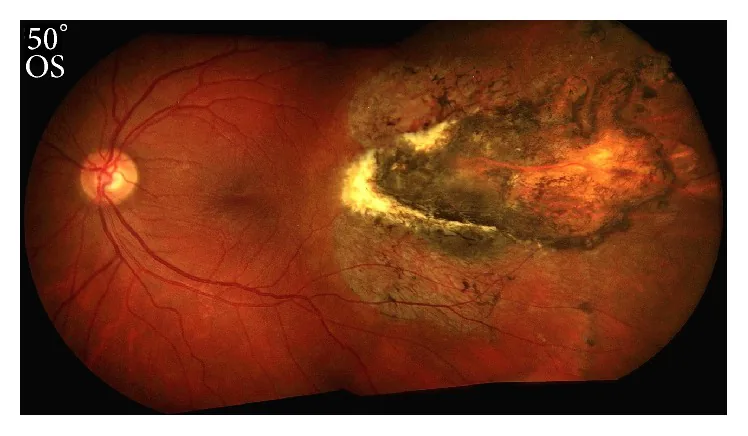
bare sclera: Visible as a white area. This is the most characteristic finding of this disease.
Choroidal rupture: Involves full-thickness defects of the choroid, Bruch’s membrane, and retina.

Chorioretinitis sclopetaria is a closed-globe ocular injury caused by the impact of a high-velocity object passing near the eye. It is characterized by full-thickness rupture of the choroid, Bruch’s membrane, and retina, exposing the bare sclera.
This disease was first described by Herman Cohn in 1872. “Sclopetaria” is derived from the Latin word “sclopetum” (handgun). In 1901, Goldzieher described it as “chorioretinitis plastica sclopetaria.”
The injury occurs as a coup injury at the impact site. This differs from the usual choroidal rupture (contrecoup injury), where the shock wave damages the opposite side.
Ordinary choroidal rupture occurs on the opposite side of the impact (contrecoup) and involves only the choroid. In contrast, chorioretinitis sclopetaria occurs at the impact site (coup) and involves full-thickness rupture of the choroid, Bruch’s membrane, and retina.
The following symptoms appear after injury.
Findings change between the acute and chronic phases.
Scleral Exposure
bare sclera: Visible as a white area. This is the most characteristic finding of this disease.
Choroidal rupture: Involves full-thickness defects of the choroid, Bruch’s membrane, and retina.
Hemorrhagic Findings
Vitreous hemorrhage: Frequently observed in the acute phase. May obstruct fundus examination.
Subretinal hemorrhage and intraretinal hemorrhage: Occur extensively around the rupture site.
Other acute phase findings
Macular edema and optic disc edema: Appear in association with inflammatory response.
RAPD and extraocular muscle palsy: Findings suggestive of damage to the optic nerve or extraocular muscles.
Elevated intraocular pressure: May occur as secondary glaucoma due to trauma.
Chronic Phase Findings
Fibroglial scar: Forms several weeks after injury.
Claw-like border: Scar with irregular borders is characteristic.
When a shock wave passes rapidly around the eyeball, its compressive force destroys the choroid and retina. Young males are the most common patient group.
Main causative objects are listed below.
| Classification | Examples |
|---|---|
| Projectiles | Air gun pellets, shot, bullets |
| Sports equipment | Paintballs |
| Others | Cork, tree branches, metal fragments |
Protective eyewear is an effective means of reducing the risk of eye injury from high-speed flying objects. However, it is difficult to completely prevent all injuries, such as those from direct impact. It is important to select protective glasses that meet appropriate standards for risky work or sports.
Diagnosis is based on trauma history and fundus findings. In the acute phase, fundus observation may be limited by vitreous hemorrhage.
The main examination methods are shown below.
| Examination Method | Main Findings |
|---|---|
| Dilated fundus examination | Scleral exposure, hemorrhage |
| OCT | Choroidal and retinal pigment epithelium rupture |
| CT | Intraorbital foreign body |
The role of each examination is as follows.
The following diseases require differentiation.
In many cases, observation is the basic approach. Extensive fibroglial proliferation often leads to spontaneous scarring and closure of retinal breaks.
Surgery is required if the following complications are present:
The main surgical procedures are as follows.
Choroidal neovascularization may develop from the scar tissue after injury. In such cases, laser photocoagulation or intravitreal injection of anti-VEGF agents is performed.
Visual prognosis is generally limited. The rate of achieving 20/20 vision is reported to be 16.4%. Ruptures involving the macula or optic nerve have a particularly poor prognosis.
In many cases, spontaneous healing due to fibroglial proliferation can be expected, so observation is the basic approach. However, surgery is necessary when complicated by retinal detachment, globe rupture, or intraocular foreign body. Regular fundus evaluation as described in Diagnosis and Examination Methods is important for early detection of complications.
The rate of achieving 20/20 vision is only 16.4%. Prognosis is particularly poor when the macula or optic nerve is involved in the rupture site, or when complicated by orbital fracture or optic neuropathy. It is difficult to predict the final outcome based solely on initial visual acuity.
When a high-speed object passes near the eye, the resulting shock wave deforms the eyeball wall, detaching and rupturing the choroid and neurosensory retina from the sclera.
Differences in the elastic properties of each tissue layer determine the rupture pattern.
Bruch's membrane
Inelasticity: Vulnerable to compressive forces, rupturing even with relatively low energy.
Rupture initiation: Rupture of Bruch’s membrane causes acute subretinal hemorrhage from the choriocapillaris.
Retinal pigment epithelium
Inelasticity: Like Bruch’s membrane, it has poor elasticity and is prone to rupture.
Hyperplasia: In the chronic phase, retinal pigment epithelium hyperplasia occurs and contributes to scar formation.
Retina and Sclera
Elasticity: Relatively high elasticity, damaged only by high-energy impact.
Scleral preservation: The sclera has the highest elasticity and is usually preserved (bare sclera).
The pathological progression after injury is as follows.
In a histopathological study by Duboby in 1974, defects in Bruch’s membrane and choroid, loss of photoreceptors, and hyperplasia of the retinal pigment epithelium were confirmed.
Traditionally, fibroglial proliferation was thought to seal the rupture site and prevent retinal detachment. However, Papakostas (2014) reported that retinal detachment was actually confirmed in a case of sclopetaria with ocular injury, questioning the conventional concept that “fibrosis prevents detachment.”
In the study by Ludwig et al., injuries from relatively low-energy objects such as air guns tended to have a poorer prognosis. Even when the impact energy was low, rupture of the temporal side or macula led to poor visual acuity, and the rate of achieving a final visual acuity of 20/20 was only 16.4% overall.
Injuries from high-energy objects (e.g., bullets) are diagnosed and treated early as globe rupture, whereas injuries from low-energy objects can damage the macula while preserving the eyeball structure, which is considered a factor contributing to poor prognosis.