Angioid streaks (AS) are a condition caused by degeneration of elastic fibers throughout the body due to a congenital predisposition. Degeneration and rupture of the elastic fibers in Bruch’s membrane result in a fundus appearance characterized by white, linear changes with pigmentation radiating from the optic disc.
This is a connective tissue disease resulting from degeneration of systemic elastic fibers. Fragility of Bruch’s membrane leads to ruptures, producing angioid streaks. First reported by Doyne in 1889, Knapp named them “angioid streaks” in 1892.
Epidemiologically, the prevalence of PXE is reported as 1:25,000 to 1:100,000, and AS appears in 85–100% of PXE patients. 2) AS is bilateral and more common in males.
A mnemonic for associated systemic diseases is PEPSI.
P: Paget disease (bone Paget disease, AS complication rate 8–15%2))
S: Sickle cell disease
I: Idiopathic
PXE is the most frequent associated disease, and the condition in which angioid streaks are complicated with PXE is called Grönblad-Strandberg syndrome. PXE is caused by mutations in the ABCC6 gene and is a systemic disease affecting three organ systems: the eyes, skin, and cardiovascular system.3) In recent years, the complication rate with Ehlers-Danlos syndrome has been reassessed and is now considered to be less than 1%.2)
Ministry of Health, Labour and Welfare PXE diagnostic criteria: PXE was designated as an intractable disease in 2015 and became eligible for medical expense subsidies.
Diagnostic item
Content
① Skin lesions
Yellow plaques in flexural areas, skin laxity, etc.
② Skin pathology
Degeneration of elastic fibers with calcification
③ Fundus findings
Presence of angioid streaks
④ Gene
ABCC6 gene mutation
Definite diagnosis: (① or ②) and ③
Suspected diagnosis: (① or ②) only, or ③ only
If a genetic mutation is confirmed in a suspected case, it is considered definitive.
QWhat systemic diseases are associated with angioid streaks?
A
PXE (pseudoxanthoma elasticum) is the most common, followed by Paget disease, sickle cell disease, and idiopathic cases. The mnemonic “PEPSI” (PXE, Ehlers-Danlos, Paget, Sickle cell, Idiopathic) is used. Angioid streaks are present in 85–100% of PXE patients. 2)
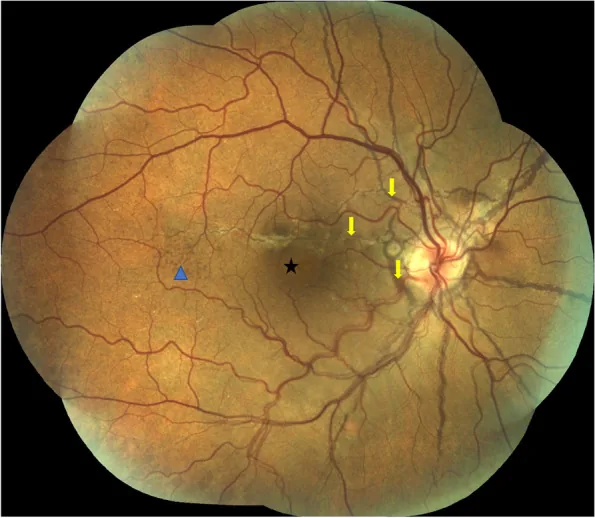
Penas SC, et al. Central serous chorioretinopathy and angioid streaks: coincidental?. BMC Ophthalmol. 2022. Figure 1. PMCID: PMC9442979. License: CC BY.
Color fundus photograph montage of the right eye. Multiple brown angioid streaks radiating from the optic disc are seen, along with a small serous detachment in the central macula and peau d’orange in the temporal mid-periphery. This corresponds to the angioid streaks discussed in section “2. Main symptoms and clinical findings.”
Angioid streaks are usually asymptomatic and are often discovered incidentally. They are frequently not accompanied by subjective symptoms until CNV develops, and may be identified during incidental ophthalmological or dermatological examinations.
The following findings are observed on slit-lamp microscopy and fundus examination.
Angioid streaks are irregular linear changes extending radially (star-shaped) from the optic disc. They usually appear white with pigmentation. They may take a flame-shaped or star-shaped form. They are typically bilateral.
Peau d’orange fundus is a characteristic finding in PXE, presenting a fundus appearance with coarse granular pigmentation from the posterior pole to the mid-periphery and yellowish-white spots in the periphery. Additionally, peripapillary chorioretinal atrophy and optic disc drusen are frequently associated.
AS alone
Peripapillary radial streaks: Linear changes radiating from the optic disc (star-shaped). White with pigmentation.
Peau d’orange fundus: Granular pigmentation and yellowish-white spots. Characteristic of PXE.
Peripapillary atrophy: Chorioretinal atrophy forms around the optic disc.
Symptoms: Usually asymptomatic. Visual acuity remains normal.
CNV Complication
Gray-white elevated lesion: Neovascularization forms on the RPE (type 2 CNV, Gass type 2). Commonly occurs in the macula and extends toward the fovea.
Subretinal hemorrhage: Bleeding in the macula due to CNV rupture. May be accompanied by serous retinal detachment or RPE detachment.
Symptoms: Metamorphopsia, central scotoma, and sudden vision loss occur.
Course: Natural prognosis is very poor. Progresses to the macula in a short period. Resistant to treatment and recurs repeatedly.
As a case report, Mandura et al. (2021) reported a 27-year-old female PXE patient with findings of 20/20 vision in both eyes, normal intraocular pressure, and no CNV or subretinal hemorrhage, indicating that PXE patients can have a course without CNV. 1)
QDoes vision decrease with angioid streaks alone?
A
Angioid streaks alone usually do not cause vision loss. Lesions away from the fovea maintain normal vision. 1) Visual impairment mainly occurs when CNV is present. Regular eye examinations are important to assess for CNV.
The underlying pathology of angioid streaks is calcification and fragility of Bruch’s membrane, and the most strongly associated disease is PXE. PXE is caused by mutations in the ABCC6 gene, and three genetic types are known. Autosomal recessive inheritance is the most common. 3)
The clinical features of each genetic type of PXE are shown below.
Genetic type
Clinical features
AR type (autosomal recessive)
Most common genetic type. Lesions in three organ systems: eyes, skin, and cardiovascular system.
AD type 1 (autosomal dominant)
Flexural rash, angina, hypertension, severe chorioretinitis
AD type 2 (autosomal dominant)
Macular rash, mild retinal degeneration
The p.R1268Q mutation in the ABCC6 gene has been reported to be associated with early onset of angioid streaks. 3)
ABCC6 encodes MRP6 (multidrug resistance-associated protein 6), which is highly expressed in the liver and kidneys, and is involved in the release of anti-calcification factors (such as inorganic pyrophosphate and fetuin A) into the blood. Genetic mutations lead to a deficiency of anti-calcification factors, causing calcium deposition in elastic tissues throughout the body. 4)
In Paget’s disease (increased bone turnover → elevated serum ALP), the rate of AS complication reaches 8–15%. 2) In sickle cell disease, the mechanism involves hemoglobin S → red blood cell deformation → iron deposition in Bruch’s membrane → weakening. 2) Blunt trauma also promotes Bruch’s membrane rupture and increases the risk of CNV development. 2)
QWhat can PXE patients do to protect their eyes?
A
Preventing Bruch’s membrane rupture due to trauma is most important. Wear rigid eye protectors during sports and avoid direct impact to the eyes. Avoid scleral compression and have regular eye exams to detect CNV early. 2)
Many cases show flat CNV spreading horizontally. During active phase: subretinal fibrin, subretinal hemorrhage, retinal edema. En face OCT is useful for layer-specific evaluation of streak lesions5)
Detects more extensive RPE damage than other observation methods. Useful for evaluating lesion extent.
OCTA: Non-invasively visualizes the microvascular structure of CNV. Useful adjunctively for monitoring CNV activity and evaluating treatment response. 6)
AMD/PCV: Beware of misdiagnosis in elderly or unilateral cases. AS-CNV occurs at a younger age than AMD and is often bilateral, which is key to differentiation.
Lacquer cracks: Bruch membrane cracks associated with high myopia. Differentiated by axial length, refractive value, and skin biopsy.
Choroidal rupture: Occurs after ocular trauma. Differentiated by history of injury.
When AS is suspected, skin inspection is important. If PXE is suspected, consult a dermatologist and consider skin biopsy. If PXE is confirmed, cardiovascular abnormalities must also be investigated.
Skin biopsy: Gold standard for PXE diagnosis. Confirms elastic fiber calcification.
ALP, Ca/P: Screening for Paget disease. 2)
Hemoglobin electrophoresis: Confirmation of sickle cell disease. 2)
QHow is angioid streaks found?
A
Since it is often asymptomatic, it is discovered incidentally during routine eye examinations or dermatology visits (when PXE is diagnosed). It may also be detected during screening eye examinations in patients with Paget disease or sickle cell disease. By the time metamorphopsia or decreased vision appears, CNV is often already present, so regular check-ups are important even in high-risk patients without symptoms.
No specific treatment is required for AS alone (without CNV), and regular follow-up is the basic approach. Provide counseling to patients on avoiding trauma. 2)
When CNV forms between the optic disc and the fovea, it tends to progress to the macula within a relatively short period. The natural prognosis is very poor, and prompt treatment initiation is necessary.
Previous treatments (limited efficacy): Neovascular removal, laser photocoagulation, photodynamic therapy (PDT), and local steroid administration have been performed, but treatment effects were limited, recurrence was frequent, and management was often difficult.
Current first-line treatment: Intravitreal anti-VEGF injection
Ranibizumab 0.5mg/0.05mL: Prospective studies (12 months) showed stable to improved mean visual acuity. Mean number of injections was 3–5 per year. 7)
Bevacizumab 1.25mg/0.05mL (off-label): Reduction in foveal thickness and stabilization of visual acuity have been reported at 6–12 months. 8)
Aflibercept 2mg/0.05mL: At 12 months, visual acuity was maintained or improved, with significant reduction in foveal thickness. 9)
Induction phase: once monthly for 3 doses, followed by PRN regimen is common. 7), 8)
Long-term prognosis shows high recurrence rates, and many cases require continued injections over several years. Reports indicate that long-term visual prognosis is limited due to progression of macular atrophy. 10)
PDT was performed for extrafoveal CNV before the anti-VEGF era, but currently anti-VEGF monotherapy is mainstream. 2)
QHow effective is treatment when choroidal neovascularization occurs?
A
Intravitreal anti-VEGF injections (ranibizumab, bevacizumab, aflibercept) have been reported to stabilize or improve vision at 12 months. 7), 8), 9) However, recurrence rates are high, and more additional doses are often required than for age-related macular degeneration. In the long term, macular atrophy may progress, leading to limited visual prognosis in some cases. 10)
Bruch’s membrane is a five-layered structure rich in elastin and collagen, located between the choriocapillaris and the RPE, and is responsible for transporting metabolites and nutrients. 2)
In PXE, mutations in the ABCC6 gene cause functional loss of MRP6, reducing secretion of anti-calcification factors such as inorganic pyrophosphate and fetuin-A from the liver. As a result, calcium deposits in elastic tissues throughout the body, and Bruch’s membrane also calcifies and weakens, leading to breaks. 4)
Type 2 CNV occurs through breaks in Bruch’s membrane and areas of RPE damage. Thickening and calcification of Bruch’s membrane are also observed in the fetal placenta, suggesting a metabolic change.
The pathology of angioid streaks progresses in stages.
Early Stage
Bruch’s membrane thickening: Calcification begins and the membrane thickens.
Decreased pigment granules: The pigment granules of the RPE decrease.
Pigment spot formation: Appears on the fundus as radial striae around the optic disc.
Symptoms: Usually asymptomatic with only striae.
End Stage
CNV development: Type 2 CNV invades through the rupture (above the RPE). It commonly occurs in the macula and progresses toward the fovea.
Subretinal hemorrhage: Bleeding occurs due to CNV rupture.
Disciform scar: Eventually, a scar forms in the macula, leading to significant vision loss.
Association with systemic diseases: PXE is caused by ABCC6 gene mutations and leads to progressive damage to elastic fibers throughout the body, including the skin, cardiovascular system, gastrointestinal tract, and placenta. It may be associated with cardiovascular diseases (angina, hypertension, peripheral artery disease, gastrointestinal bleeding), and evaluation by a cardiologist in addition to a dermatologist should be considered. 2)
Pathologically, extensive calcification and thickening of Bruch’s membrane are observed. At the rupture site, the RPE becomes thin, and fibrovascular tissue invades, leading to subretinal hemorrhage, CNV, and disciform scar formation. 2)
7. Latest research and future perspectives (reports at the research stage)
AS-CNV has a higher recurrence rate compared to AMD-CNV, and the need for more aggressive dosing regimens is being discussed. In long-term (over 5 years) outcomes, many cases have limited visual prognosis due to progression of macular atrophy, and development of treatments to suppress atrophy progression is a future challenge. 10)
Advances in OCTA have enabled detailed structural evaluation of CNV, and it is expected to improve the accuracy of treatment effect assessment and recurrence detection. 6) Layer-by-layer evaluation of angioid streak lesions using en face OCT has also been reported. 5)
Clinical trials of anti-calcification treatments such as inorganic pyrophosphate supplementation and etidronate have been reported for PXE caused by ABCC6 gene mutations.
Kranenburg et al. (2018) conducted an RCT to evaluate the effect of etidronate (bisphosphonate) on suppressing ectopic calcification progression in PXE patients. 11) Suppression of progression was confirmed in some calcifications, but further research is needed to establish efficacy.
Pathological analysis of PXE using mouse models (Abcc6-/-) is progressing, and basic research on gene therapy and molecular targeted therapy is also being developed. 4)
Georgalas I, Papaconstantinou D, Koutsandrea C, et al. Angioid streaks, clinical course, complications, and current therapeutic management. Ther Clin Risk Manag. 2009;5(1):81-89.
Chassaing N, Martin L, Calvas P, et al. Pseudoxanthoma elasticum: a clinical, pathophysiological and genetic update including 11 novel ABCC6 mutations. J Med Genet. 2005;42(12):881-892.
Li Q, Jiang Q, Pfendner E, et al. Pseudoxanthoma elasticum: clinical phenotypes, molecular genetics and putative pathomechanisms. Exp Dermatol. 2009;18(1):1-11.
Takeuchi T, Hirai H, Ogata N, et al. En-face optical coherence tomography is useful for assessing striated lesions in angioid streaks: a case report. Cureus. 2023;15(9):e45983.
Corbelli E, Carnevali A, Marchese A, et al. Optical coherence tomography angiography features of angioid streaks. Retina. 2018;38(11):2128-2136.
Ladas ID, Kotsolis AI, Ladas DS, et al. Intravitreal ranibizumab treatment of macular choroidal neovascularization secondary to angioid streaks: one-year results of a prospective study. Retina. 2010;30(8):1227-1233.
Tilanus MA, Cuypers MH, Bemelmans NA, et al. Intravitreal bevacizumab in the treatment of choroidal neovascularization associated with angioid streaks. Acta Ophthalmol. 2007;85(8):918-920.
Esen E, Sizmaz S, Demircan N. Intravitreal aflibercept for management of subfoveal choroidal neovascularization secondary to angioid streaks. Indian J Ophthalmol. 2015;63(7):616-618.
Gliem M, Finger RP, Fimmers R, et al. Treatment of choroidal neovascularization due to angioid streaks: a comprehensive review. Retina. 2013;33(7):1300-1314.
Kranenburg G, de Jong PA, Bartstra JW, et al. Etidronate for prevention of ectopic mineralization in patients with pseudoxanthoma elasticum. J Am Coll Cardiol. 2018;71(10):1117-1126.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.