Paraneoplastic syndromes (PNS) are a group of disorders caused by a host immune response against tumor-associated antigens that cross-react with normal tissues, rather than direct effects of the cancer or its metastases. In ophthalmology, various sites such as the retina, optic nerve, and ocular motor system can be affected.
The main types of ophthalmic PNS are as follows:
CAR (cancer-associated retinopathy): Primarily involves damage to rod photoreceptors. A protein specific to the central nervous system is ectopically expressed in tumor tissue, triggering autoimmunity that damages the retinal visual system.
The main malignancy associated with CAR is small cell lung cancer, followed by gastrointestinal and gynecological cancers. There is no gender difference. MAR is caused only by malignant melanoma, and cases have been reported in Japan. Other PNS are associated with non-small cell lung cancer, breast cancer, uterine cancer, thyroid cancer, lymphoma, etc.
The onset time varies depending on the type of cancer. In lymphoma and lung cancer, retinopathy develops within weeks to months, whereas in breast and prostate cancer, it may take several years.
QCan eye symptoms appear before a cancer diagnosis?
A
In CAR, eye symptoms appear before the cancer diagnosis in about 50% of cases. Unexplained progressive vision loss may lead to further examination and discovery of a malignant tumor.
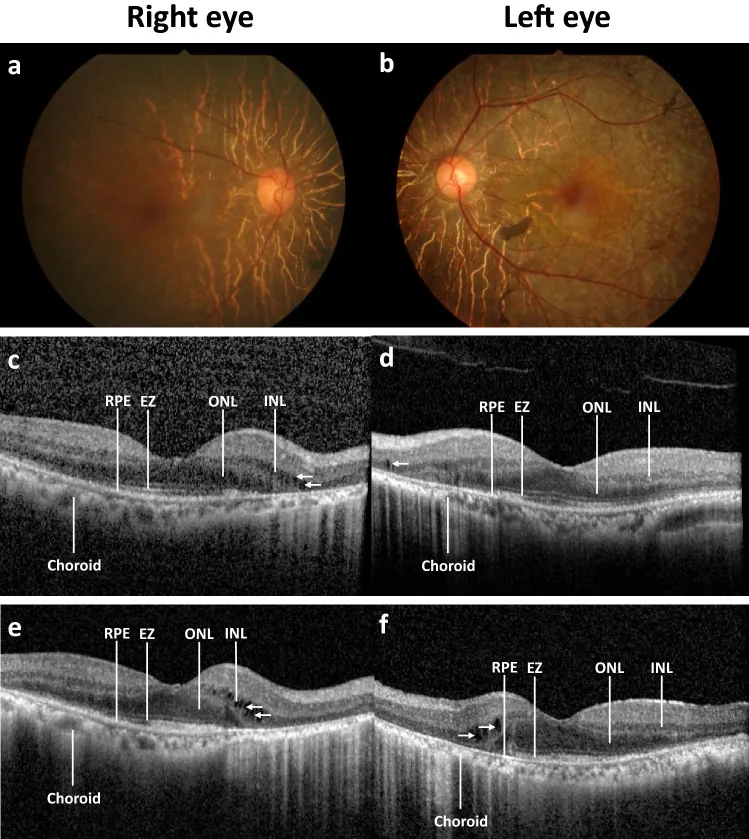
Autoantibody profiles and clinical association in Thai patients with autoimmune retinopathy. Sci Rep. 2021 Jul 22; 11:15047. Figure 1. PMCID: PMC8298708. License: CC BY.
Disease progression of a patient with autoimmune retinopathy (AIR). Color fundus photography at baseline in the right (a) and left eye (b) shows normal optic disc, arteriolar attenuation, generalized retinal pigment epithelium (RPE) atrophy with macular sparing and scattered pigment clumps. Prominent large choroidal vessels can be observed around the optic disc. Optical coherence tomography images at baseline showing RPE attenuation, loss of ellipsoid zone (EZ) at the periphery, flattening of the outer nuclear layer (ONL), and slit cavitation in the inner nuclear layer (INL) on the nasal side, as marked by arrows, in the right (c) and left eye (d). The disease progression after five years is marked with RPE atrophy, progressive loss of EZ and ONL toward the fovea, more prominent slit cavit
The pathogenesis of PNS involves an autoimmune mechanism in which nervous system antigens ectopically expressed in tumor tissue are recognized by the immune system. Autoantibodies against tumor-associated antigens are produced and attack normal nerve and retinal tissues that express the same antigens.
The main causative malignancies and associated disease types are as follows:
Small cell lung cancer: The most common cause of CAR, PON, and anti-Hu antibody-associated syndromes.
Malignant melanoma: The sole cause of MAR.
Non-small cell lung cancer, breast cancer, uterine cancer, thyroid cancer: Associated with CAR and other PNS.
Neuroblastoma (pediatric): A representative cause of paraneoplastic opsoclonus.
The basis of diagnosis is a combination of clinical symptoms, ophthalmologic findings, and identification of causative autoantibodies. Since ocular symptoms precede cancer diagnosis in about 50% of CAR cases, prompt recognition of this condition can also lead to early cancer detection.
The following findings raise suspicion for this condition.
When a patient aged 50 years or older without a family history presents with fundus findings resembling retinitis pigmentosa and visual field constriction.
When there is marked visual field constriction and decreased light sensitivity despite mild uveitis.
Antibody detection by immunohistochemical staining assay, Western blot, and ELISA is necessary for definitive diagnosis. The presence of anti-recoverin antibodies is strong evidence for CAR. For a definitive diagnosis of MAR, demonstration of serum anti-retinal bipolar cell antibodies is required.
Antibodies may not be detected on initial testing. At least three or more repeated measurements are necessary.
CT, MRI, PET: Used to search for the primary tumor.
Cerebrospinal fluid (CSF) analysis: to evaluate nervous system involvement.
Serum testing for paraneoplastic antibodies: comprehensive search for associated antibodies such as anti-Ri, anti-Hu, anti-Yo, and anti-Ma2.
Since ocular symptoms often precede the primary tumor, when this condition is suspected, a thorough systemic examination of the respiratory, gastrointestinal, urological, and gynecological systems is essential.
The most important differentiating point is the electroretinogram pattern. CAR shows overall flattening with reduction of both a-wave and b-wave, whereas MAR is characterized by a negative electroretinogram with nearly normal a-wave and markedly reduced b-wave, reflecting bipolar cell dysfunction.
Treatment of the underlying malignant tumor is the highest priority. No definitive treatment for CAR and MAR has been established, and there are no controlled human studies showing improvement in visual symptoms.
There is no indication for ophthalmic surgery for PNS. Resection of the underlying malignancy is the treatment for the underlying disease. For PNS associated with thymoma, there is evidence that thymectomy improves symptoms.
QIs there an established treatment for ocular symptoms of paraneoplastic syndrome?
A
No established treatment exists. Treatment of the underlying malignancy is the highest priority. Immunosuppressive therapy, IVIG, and plasma exchange have been attempted, but only case reports of success exist, with no controlled studies. Patients should be informed that the visual prognosis is generally poor.
Malignant tumors ectopically express proteins specific to the nervous system (such as recoverin). The immune system recognizes these as tumor antigens and produces specific antibodies. These antibodies cross-react with the same antigens on retinal photoreceptor cells, causing photoreceptor degeneration and apoptosis.
The main autoantibodies and targets reported in CAR are as follows.
Autoantibody
Main target cells
Main associated cancer
Anti-recoverin
Rod and cone photoreceptors
Small cell lung cancer
α-Enolase
Retinal ganglion cells and bipolar cells
Small cell lung cancer
Anti-hsc70
Photoreceptor cells
Various cancers
Alpha-enolase antibodies induce death of retinal ganglion cells and bipolar cells via apoptosis.
Mechanism of CRMP-5-related optic neuropathy (PON)
CRMP-5 (CV2)-IgG antibodies present with a wide range of peripheral and central nervous system phenotypes, typically paraneoplastic, with small cell lung cancer being the most common 1). In CRMP-5-related optic neuritis, bilateral optic disc edema is characteristic, accompanied by retinitis and vitreous inflammatory cells 2). The most common mechanism as optic neuritis is considered to be photoreceptor apoptosis via a cascade-dependent pathway involving intracellular calcium influx.
There are also case reports of optic neuritis involving anti-recoverin antibodies 3).
Anti-Hu antibody: Affects the brainstem, cerebellum, and temporal lobe, presenting with tonic pupil and ophthalmoplegia. Typical in small cell lung cancer.
Anti-Yo antibody: Primarily affects the cerebellum, presenting with OMS-related findings (nystagmus, oscillopsia).
Anti-AChR and striated muscle antibodies: Present with myasthenia gravis (MG)-like diplopia and ptosis associated with thymoma.
VGCCA: Associated with LEMS, presenting with mild dry eye and ocular motor abnormalities.
QWhich autoantibodies cause ocular symptoms?
A
Anti-recoverin, α-enolase, and hsc70 are involved in CAR, and CRMP-5 is a representative causative antibody for PON. Additionally, anti-Hu, anti-Yo, anti-AChR, and VGCCA antibodies correspond to each disease type. Symptom patterns and associated cancers differ depending on the type of autoantibody (see “Diagnosis and Testing Methods” section for details).
7. Latest Research and Future Perspectives (Research-stage Reports)
Kaushik et al. (2024) reported a case of anti-recoverin antibody-positive optic neuritis that responded to a combination of chemotherapy, steroids, and plasma exchange 3). Although not an established standard treatment, it is noted as an example suggesting the potential effectiveness of a multifaceted therapeutic approach.
In a rat model of CAR, calcium channel blockers have been suggested to be effective. This finding indicates the involvement of intracellular calcium influx in photoreceptor apoptosis and may serve as a basis for future treatment development.
Relationship between tumor immunity and visual prognosis
It has been suggested that tumors with PNS may have a better prognosis than those without PNS. The autoimmune response may simultaneously function as antitumor immunity, and an association with early cancer detection has been suggested. On the other hand, visual prognosis is generally poor, and the unpredictable course despite various treatments remains a challenge.
Wang S, Hou H, Tang Y, et al. An overview on CV2/CRMP5 antibody-associated paraneoplastic neurological syndromes. Neural Regen Res. 2023;18:2357-64.
Cross SA, Salomao DR, Parisi JE, et al. Paraneoplastic autoimmune optic neuritis with retinitis defined by CRMP-5-IgG. Ann Neurol. 2003;54:38-50.
Kaushik M, Virdee J, Giridharan S, Chavda SV, Batra R. Response of Recoverin-Positive Optic Neuritis to Chemotherapy, Steroid, and Plasma Exchange. Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society. 2024;44(1):e79-e81. doi:10.1097/WNO.0000000000001778. PMID:36729925.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.