Neuroblastoma (NB) is a malignant tumor arising from sympathetic nervous system precursor cells derived from the neural crest. It accounts for approximately 10% of childhood malignant tumors and is the most common extracranial solid tumor in children. It is also the second most common malignant tumor after leukemia.
Primary sites include the adrenal gland in about 46% of cases, abdomen (extra-adrenal) in about 18%, posterior mediastinum in about 14%, and pelvis/other in about 22% 4). More than 60% occur in the abdomen, such as the adrenal gland or sympathetic ganglia.
Epidemiological features are as follows:
Approximately 700 cases are diagnosed annually in the United States
Median age at diagnosis is 19 months. 90% are diagnosed before age 5 5)
Occurrence in adults is extremely rare, at 1 per 10 million people per year 5)
Ophthalmologically, 11–56% of neuroblastomas metastasize to the orbit. Clinical presentations range from spontaneous regression to extensive metastasis.
Historical background is as follows:
1864: Virchow first reported an abdominal tumor as “glioma”
1891: Marchand described features originating from the adrenal medulla and sympathetic nervous system
1901: Pepper reported infant cases with liver metastasis (equivalent to current Stage MS)
1910: Homer Wright described Homer-Wright pseudorosettes in the bone marrow
QWhere does neuroblastoma commonly metastasize?
A
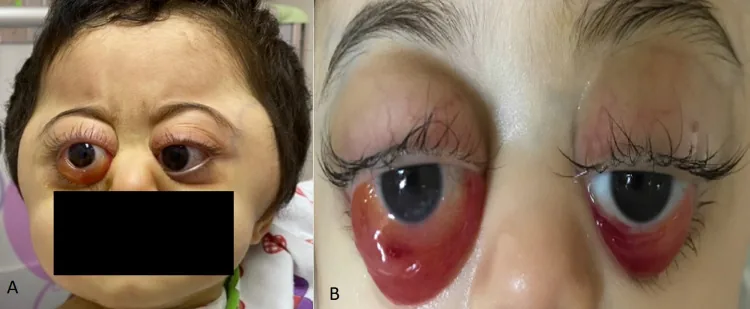
Metastases are common to bones, bone marrow, lymph nodes, liver, and skin. Orbital metastasis occurs in 11–56% of cases, and proptosis or periorbital ecchymosis (raccoon eyes) may be the initial symptom.
Rahaf A Mandura. Rapidly Progressive Ocular Proptosis as the First Sign of Neuroblastoma in a 16-Month-Old Child: Case Report and Review of Literature. Cureus. 2022 Jan 6; 14(1):e20982. Figure 1. PMCID: PMC8817620. License: CC BY.
They are divided into ophthalmic findings associated with orbital metastasis and neurological findings due to the tumor.
Orbital and periorbital findings
Periorbital ecchymosis (raccoon eyes): The most common finding in orbital metastasis in children under 2 years old. It results from hemorrhagic necrosis of the tumor. It is easily mistaken for child abuse.
Proptosis: Forward displacement of the eye due to an intraorbital tumor mass.
Eyelid and conjunctival edema: Edema may become prominent.
Eyelid ecchymosis: A characteristic finding in NB and leukemia.
Orbital bone destruction: Osteolytic changes confirmed by imaging.
Neurological and fundus findings
Horner syndrome: Triad of miosis, ptosis, and anhidrosis. Occurs when a primary thoracic tumor involves the sympathetic chain.
Heterochromia iridis: Seen in Horner syndrome due to congenital cervical ganglion NB.
Lateral rectus palsy, strabismus, esotropia: Due to impaired eye movement.
Papilledema, retinal hemorrhage, optic atrophy: Due to increased intracranial pressure or direct infiltration.
QIf a child has bruise-like bleeding around the eyes, could it be neuroblastoma?
A
Periorbital subcutaneous hemorrhage (raccoon eyes) is the most common finding in orbital metastasis in children under 2 years of age. Bilateral periorbital hemorrhage without a history of trauma should raise strong suspicion for neuroblastoma. Since it is easily mistaken for child abuse, systemic evaluation including abdominal ultrasound and urinary catecholamine testing is necessary for differential diagnosis.
QWhat is opsoclonus-myoclonus syndrome?
A
This syndrome is characterized by high-frequency (10–15 Hz), multidirectional saccadic eye movements accompanied by myoclonus. It is considered a paraneoplastic syndrome caused by abnormal antibodies against neuronal RNA. Latent neuroblastoma is present in 48% of patients with OMS, and systemic evaluation is essential in children with OMS.
The majority of cases are sporadic, and no clear risk factors have been identified.
Genetic factors (approximately 1–2% of all cases):
ALK germline mutation: Most common cause of familial NB
PHOX2B abnormality: Associated with impaired differentiation into mature neurons
KIF1B abnormality / MYCN amplification: Part of familial NB
NBPF10 copy number variation (1p/11q deletion): Associated with high-risk NB
LMO1 gene duplication: Risk factor for aggressive NB
Association with NF1 and Beckwith-Wiedemann syndrome: Rarely co-occurs
Genetic mutations associated with sporadic NB:
Genetic variation at 6p22: Reported to be associated with sporadic NB
MYCN amplification is found in 20–25% of childhood NB and shows a bimodal distribution of 3–10-fold or 100–300-fold. It is a molecular marker strongly associated with aggressive NB5).
Molecular biological features of adult NB differ from those in children; MYCN amplification is rare. ATRX mutations (11%), ALK mutations (up to 14%), and TERT rearrangements (23%) are characteristic5).
Urinary catecholamines (HVA/VMA): Previously reported to be elevated in 90–95% of cases, but recent studies show lower sensitivity. In adults, it is only 40–57% (in contrast to 95% in children).
The characteristics of each modality are shown below.
Test
Characteristics
Indications
CT
Well-defined/ill-defined, high attenuation, microcalcifications
Initial evaluation, orbital osteolytic changes
MRI
T1 hypointense, T2 heterogeneous, evaluation of intracranial extension
Detailed intracranial and orbital examination
MIBG (123I)
Optimal for identifying soft tissue and bone metastases
Whole-body assessment of metastases
PET
High sensitivity and specificity
Diagnosis and treatment monitoring
MIBG scintigraphy (123I-MIBG) is superior to PET/CT in identifying soft tissue and bone metastases. In orbital metastases, CT shows osteolytic changes, and MRI shows isointensity to extraocular muscles and hypointensity to fat on T1-weighted images, and hyperintensity to extraocular muscles and fat on T2-weighted images. Metastases to the posterolateral wall of the orbit are common.
QWhat is the most useful imaging test for neuroblastoma?
A
MIBG scintigraphy (123I-MIBG) is considered the most useful for identifying soft tissue and bone metastases, and is superior to PET/CT. Because it can evaluate all metastatic lesions throughout the body at once, it is used for both initial staging and treatment response assessment.
Total resection is rarely indicated for metastatic orbital tumors. Treatment effective for the primary cancer, such as chemotherapy or radiation therapy, is performed. In pediatric neuroblastoma, if the tumor responds to chemotherapy, the prognosis is relatively good. The 5-year survival rate with orbital metastasis is very poor at 7.6%.
There is no established standard protocol, and pediatric protocols are often adapted5). Surgery (including laparoscopic) + chemotherapy (such as carboplatin + etoposide) is performed. The 5-year overall survival rate for adults aged 20 years or older is 36.3%, indicating a poor prognosis5).
QWhat is the prognosis when neuroblastoma metastasizes to the orbit?
A
The 5-year survival rate for neuroblastoma with orbital metastasis is very poor at 7.6%. Orbital metastasis often indicates distant metastasis (equivalent to Stage M), and multidisciplinary treatment is performed as a high-risk group, but there are limits to improving prognosis.
NB arises from sympathetic nervous system precursor cells (sympathoblasts). PHOX2B mutations impair differentiation into mature neurons, leading to tumorigenesis. ALK mutations are associated with reduced proliferation and an increase in immature sympathetic neurons.
Catecholamine metabolism abnormality: Due to defective catecholamine synthesis in tumor cells, intermediate metabolites HVA and VMA accumulate and are excreted in urine. This forms the basis for urinary catecholamine testing.
Opsoclonus-myoclonus syndrome (OMS): Caused by abnormal antibodies against neuronal RNA. It is considered a paraneoplastic symptom due to cross-reactivity with tissue.
Mechanism of visual impairment (without direct compression): Immune response to NB cross-reacts with tissue. Cancer-derived toxic metabolites and chemotherapy-induced axonal transport stasis may also be involved.
Some NB (especially Stage MS) undergo spontaneous regression. Mechanisms are thought to involve subtelomeric DNA hypermethylation, apoptosis, nerve growth factor (NGF) deficiency, and immune response.
Molecular Biological Characteristics of Pediatric vs. Adult NB
Children and adults have significantly different genetic characteristics1)5).
Feature
Pediatric NB
Adult NB
MYCN amplification
20–25%
Rare
PHOX2B expression
High (high sensitivity and specificity)
50% negative
ATRX mutation
Rare
11%
ALK mutation
Rare
Up to 14%
TERT rearrangement
Rare
23%
The fact that 50% of adult NB are PHOX2B-negative suggests the possibility of a different cell lineage (such as thymic origin) compared to the pediatric type1).
7. Latest Research and Future Perspectives (Investigational Reports)
On December 13, 2023, the US FDA approved a new drug for maintenance therapy of high-risk NB3).
Jiang & Yu et al. (2024) detailed the pharmacological profile of eflornithine, reporting it as an irreversible inhibitor (suicide inhibitor) of ODC (ornithine decarboxylase), targeting the polyamine pathway in MYCN-amplified NB3). A Phase 2 trial (NCT02395666) as maintenance therapy after immunotherapy (dinutuximab) was completed, leading to FDA approval.
Drug properties:
Molecular weight: 182.2 g/mol
Route of administration: Oral
Half-life: Approximately 3.5 hours (renal excretion, almost not metabolized)
Indication: maintenance therapy after immunotherapy for high-risk neuroblastoma
Main side effects: fever, infections, allergic reactions, cough, conjunctival hyperemia, liver toxicity, hearing loss, diarrhea, nausea, vomiting3)
Personalized treatment strategies using digital therapy planning (e.g., Oncompass™) are being explored5).
QWhat is eflornithine (IWILFIN)?
A
It is an oral drug approved by the FDA in December 2023 as maintenance therapy after immunotherapy for high-risk neuroblastoma. It irreversibly inhibits ODC (ornithine decarboxylase), suppressing polyamine synthesis and blocking tumor growth signals driven by MYCN amplification 3). Approval status in Japan should be confirmed with the attending physician.
Collins K, Ulbright TM, Davis JL. Anterior mediastinal neuroblastoma in an adult: an additional case of a rare tumor in an unusual location with review of the literature. Diagn Pathol. 2023;18:127.
Hu J, Xia B, Yuan X, et al. Neuroblastoma with superficial soft tissue mass as the first symptom: case reports with atypical ultrasonic image and literature review. Braz J Med Biol Res. 2023;56:e12975.
Jiang J, Yu Y. Eflornithine for treatment of high-risk neuroblastoma. Trends Pharmacol Sci. 2024;45(6):577-578.
do Amaral-Silva GK, Leite AA, Mariz BALA, et al. Metastatic neuroblastoma to the mandible of children: report of two cases and critical review of the literature. Head Neck Pathol. 2021;15:757-768.
Telecan T, Andras I, Bungardean MR, et al. Adrenal gland primary neuroblastoma in an adult patient: a case report and literature review. Medicina. 2023;59:33.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.