Multiple myeloma (MM) is a malignant disease in which plasma cells that produce immunoglobulins (Ig) proliferate uncontrollably. It accounts for about 10% of hematologic malignancies, with a median age at diagnosis of 65 to 70 years. It is more common in men over 50.
MM is a systemic disease and presents a variety of ocular symptoms involving the eyelids, iris, cornea, retina, optic nerve, and brain. There are two main mechanisms of ocular symptoms.
Direct infiltration: Compression and destruction of intraocular and periorbital structures by plasmacytoma masses.
Hyperviscosity: Increased blood viscosity due to abnormal immunoglobulin elevation. Causes stasis and occlusion of retinal vessels.
Neuro-ophthalmic findings are the most common, occurring in about 50% of MM patients. Orbital infiltration can be an initial sign of MM, so ophthalmologists may be the first to detect systemic disease. Under modern treatment, median survival is about 7–8 years, but in cases with hyperviscosity syndrome, survival is reportedly shortened to about 3.6 years.
QHow often do eye symptoms occur in multiple myeloma?
A
Neuro-ophthalmic findings are the most common ocular complication of MM, seen in about 50% of patients. Since orbital infiltration can be the first symptom of MM, systemic evaluation is important for unexplained eye symptoms.
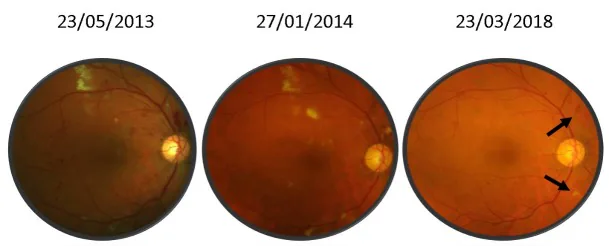
Monica Malaescu, Bogdana Tabacaru, Simona Stanca et al. Bilateral Central Retinal Vein Occlusion, multiple dental implants and severe glomerulonephtitis – Any connection?. Romanian Journal of Ophthalmology. 2019 Jul-Sep; 63(3):287. Figure 2. PMCID: PMC6820500. License: CC BY.
Figure 1: Changes in the number of patients from 2013 to 2018 (source: Ministry of Health, Labour and Welfare Patient Survey)
Many patients are asymptomatic in the early stages, and even without symptoms, many ocular complications may be lurking. When symptoms appear, the following are common.
Diplopia: Caused by impaired eye movement due to abducens nerve or oculomotor nerve damage.
Eye pain or pressure sensation: Pain due to intraorbital mass or bone destruction.
QWhat are the characteristic fundus findings of hyperviscosity retinopathy?
A
Bilateral involvement, dilation and tortuosity of retinal veins (sausage-like changes), and scattered multiple blot and flame-shaped hemorrhages are characteristic findings. In advanced cases, optic disc swelling and serous retinal detachment may also occur. Differentiation from diabetic retinopathy (with hard exudates) and hypertensive retinopathy (predominantly linear hemorrhages) is important.
The underlying cause of MM is uncontrolled proliferation of plasma cells, and the following two mechanisms lead to ocular symptoms.
Direct infiltration: The plasmacytoma mass compresses and destroys surrounding structures.
Hyperviscosity: Increased abnormal immunoglobulins raise blood viscosity. When blood viscosity exceeds 4 centipoise, intraocular thrombotic events may occur.
Risk factors for developing MM include exposure to ionizing radiation, benzene, and herbicides. Additionally, a precursor condition called MGUS (monoclonal gammopathy of undetermined significance) exists, which progresses to MM at a rate of about 1% per year.
Systemic symptoms include the three major symptoms of anemia, back pain, and proteinuria, as well as hypercalcemia, renal dysfunction, increased susceptibility to infections, osteolytic lesions, and pathological fractures.
QCan eye symptoms be the first sign of multiple myeloma?
A
Orbital infiltration can be the initial symptom of MM, and an ophthalmological diagnosis may lead to the discovery of systemic disease. For ocular findings suggestive of systemic disease, such as bilateral retinal changes or proptosis, active collaboration with hematology should be considered.
Fundus examination and fundus photography: Detect findings characteristic of MM, such as retinal hemorrhage, venous dilation, and papilledema.
Fluorescein angiography (FA): Perform qualitative diagnosis of avascular areas due to capillary occlusion, delayed dye inflow, and perfusion defects. Retinal vein dilation and leakage from peripheral vessels can also be confirmed.
The diagnosis of MM is primarily handled by hematology, but it is important for ophthalmologists to understand the basic examination system.
Urine test: The presence or absence of Bence Jones protein is important for diagnosis. Perform urine protein electrophoresis (UPEP) and immunofixation using 24-hour urine collection.
Blood test: Detection of erythrocytosis, M protein, and hypergammaglobulinemia. Complete blood count, peripheral blood smear, and basic metabolic panel.
Serum protein electrophoresis (SPEP) and immunofixation: Detect M protein of abnormal immunoglobulins.
Bone marrow biopsy: Confirms abnormal proliferation of plasma cells. Essential for definitive diagnosis.
Skeletal survey: X-ray examination for osteolytic lesions throughout the skeleton.
Differential diagnosis of systemic diseases: Smoldering multiple myeloma, MGUS, POEMS syndrome, solitary plasmacytoma, plasma cell leukemia, AL amyloidosis.
Differential diagnosis of fundus hemorrhage: Distinguish from diabetic retinopathy (with cotton-wool spots and hard exudates) and hypertensive retinopathy (mainly linear hemorrhages). Bilateral involvement and sausage-like venous changes suggest MM.
Chemotherapy: Melphalan was traditionally used. Currently, combination with steroids and hematopoietic stem cell transplantation are standard.
Molecular targeted drugs: Bortezomib (proteasome inhibitor), thalidomide (with anti-angiogenic effect), and lenalidomide (a thalidomide derivative with reduced side effects) are used.
Examples of main drug combinations:
Lenalidomide + low-dose dexamethasone
Bortezomib + dexamethasone
Bortezomib + thalidomide + dexamethasone
Vincristine + doxorubicin + dexamethasone
For patients not at high risk: Melphalan + prednisone + thalidomide for 12 cycles, then observation.
High-risk patients: Evaluate eligibility for bone marrow transplantation after 2–4 cycles of non-alkylator-based induction therapy.
Asymptomatic MM: Active treatment may not be necessary.
Plasmapheresis (blood purification): Performed for hyperviscosity syndrome.
Other supportive therapies: Preventive treatment for hypercalcemia, bone disease, and infections is also required.
Conjunctival cell infiltration: Systemic chemotherapy is effective.
Retinal avascular zone/retinal ischemia: Perform scatter laser photocoagulation (under mydriasis) to prevent retinal neovascularization and vitreous hemorrhage.
Antiplatelet therapy/anticoagulation therapy: Consider when there is retinal vein dilation, tortuosity, or CRVO-like findings.
Vitrectomy: Performed when vitreous hemorrhage does not resolve spontaneously.
Shared management: An ophthalmologist suspecting MM should refer the patient to a hematologist. It is important for the ophthalmologist to regularly evaluate ocular symptoms and communicate closely with the internist.
QWhat ophthalmologic treatments are performed for ocular symptoms of multiple myeloma?
A
Radiation therapy (20–40 Gy) is used for orbital infiltration. Laser photocoagulation is performed for retinal avascular zones associated with hyperviscosity retinopathy to prevent neovascularization and vitreous hemorrhage. Vitrectomy is performed if vitreous hemorrhage does not resolve spontaneously. Anticoagulation therapy is considered for findings resembling retinal vein occlusion. All treatments are based on collaboration with the hematology department.
Plasma cells differentiate from B lymphocytes and produce immunoglobulins. Immunoglobulins consist of two heavy chains (IgG, IgM, IgA, IgE, IgD) and two light chains (κ or λ). In MM, IgG or IgA levels are usually elevated.
As the disease progresses, light chains are overproduced relative to heavy chains. The severity can be assessed by monitoring the κ/λ ratio.
Direct infiltration: Tumor formation compresses and destroys surrounding structures. This causes proptosis due to orbital bone destruction, diplopia due to nerve compression, and decreased visual acuity.
Hyperviscosity: According to Poiseuille’s law, intravascular flow resistance increases proportionally to viscosity. When blood viscosity exceeds 4 centipoise, thrombotic events in the eye may occur. Increased serum viscosity and vascular endothelial cell damage caused by pathological proteins are the main causes of fundus lesions.
Ripa M, Schipa C, Aceto P, Shah NA. Exploring the ocular involvement in multiple myeloma: a comprehensive review of 70-year clinical studies. Int Ophthalmol. 2025;45(1):89. PMID: 40085267
Chin KJ, Kempin S, Milman T, Finger PT. Ocular manifestations of multiple myeloma: three cases and a review of the literature. Optometry. 2011;82(4):224-230. PMID: 21193351
Kuo HH, Shen EP. Hyperviscosity retinopathy as the initial presentation of aggressive multiple myeloma. Tzu Chi Med J. 2020;32(4):401-403. PMID: 33163389
Tandlich MA, Williamson K. Bilateral Central Retinal Vein Occlusion as a First Presentation of Multiple Myeloma: A Case Report. Clin Pract Cases Emerg Med. 2022;6(3):232-235. PMID: 36049195
Wang SSY, Lee MB, George A, et al. Five cases of orbital extramedullary plasmacytoma: diagnosis and management of an aggressive malignancy. Orbit. 2019;38(3):218-225. PMID: 29985709
Debureaux PE, Harel S, Parquet N, et al. Prognosis of hyperviscosity syndrome in newly diagnosed multiple myeloma in modern-era therapy: A real-life study. Front Immunol. 2022;13:1069360. PMID: 36569885
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.