Cysticercosis is an infectious disease caused by the larval stage of the pork tapeworm (Taenia solium), known as Cysticercus cellulosae, which parasitizes tissues. Humans are typically the definitive host, but if they accidentally ingest eggs, they become an intermediate host and develop cysticercosis.
When the central nervous system is affected, it is called neurocysticercosis (NCC). NCC is a leading cause of adult-onset epilepsy worldwide, and the WHO considers it a major public health concern. The CDC has designated it as a neglected parasitic infection.
When the eye or orbit is affected, it is called ocular or orbital cysticercosis (OOC). OOC is considered a preventable cause of blindness.
Endemic areas include Southeast Asia, the Indian subcontinent, Central and South America, and Africa, where sanitation is poor. In the United States, there are approximately 1,000 new hospitalizations due to NCC each year, and 10% of emergency visits for seizures in the Southwest are attributed to cysticercosis. Most cases in the US are among immigrants from Central and South America.
The distribution of cysticercosis by site of infection is reported as follows:
Subretinal space: 35%
Vitreous body: 22%
Subconjunctival space: 22%
Anterior segment: 5%
Orbit: 1%
In India, the ocular adnexa (orbital adnexal tissues) are the most common site of involvement. In Europe and the United States, the posterior pole of the eye is the primary site of infection.
QIn which regions is ocular cysticercosis common?
A
It is prevalent in areas with poor sanitation, such as Southeast Asia, the Indian subcontinent, Central and South America, and Africa. In the United States, cases are increasing, particularly among immigrants from Central and South America, with approximately 1,000 new NCC hospitalizations per year.
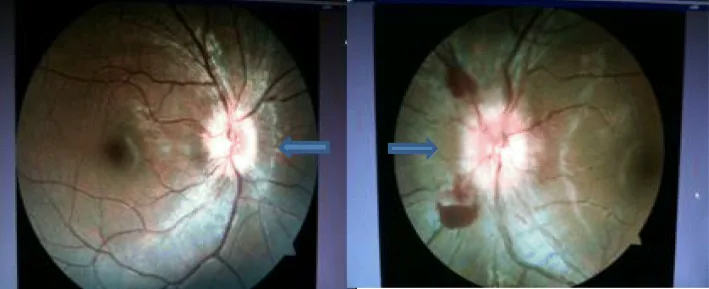
Ruchi Shrestha, Amin Kumar Shrestha. Disseminated neurocysticercosis with bilateral papilledema: a case report. Journal of Medical Case Reports. 2019 Sep 18; 13:295. Figure 2. PMCID: PMC6749648. License: CC BY.
When NCC is present, it may cause seizures/epilepsy, stroke due to cerebral infarction, cognitive decline, and neuropsychiatric disorders.
Extraocular muscle cysticercosis presents with nonspecific symptoms such as recurrent swelling, eyelid edema, and eye movement disorders, and may be misdiagnosed as pseudotumor leading to steroid administration1).
Clinical Findings (Findings Confirmed by Physician Examination)
Optic disc edema: Due to compression of the optic nerve. Rare.
Subconjunctival and orbital
Subconjunctival cysticercus: Recognized as a raised red to yellow nodular mass.
Proptosis and eyelid swelling: Findings of orbital cysticercosis. May be accompanied by ocular muscle palsy.
Extraocular muscle thickening: Most commonly affects the superior rectus. Cysticercus and scolex can be confirmed by ultrasound1).
If symptoms suggest brain lesions, a complete neurological examination is necessary. Papilledema, cranial nerve palsy, stroke signs, and meningeal irritation signs may be present.
Cysticercosis develops when humans ingest eggs of the pork tapeworm. There are three routes of infection.
Heterologous infection: Ingestion of food or water contaminated with eggs.
Autoinfection: Self-ingestion of eggs excreted from existing parasites.
Endogenous autoinfection: Mature proglottids are carried from the intestine to the stomach by reverse peristalsis, releasing eggs.
After ingestion, the protective capsule of the eggs is dissolved by gastric acid. After maturing into larvae, they travel through the bloodstream to tissues such as the brain, eyes, and striated muscle.
Risk factors include the following1).
Poor sanitation: Inadequate water and sewage infrastructure.
Pig farming environment: Free-range farming in endemic areas.
Consumption of undercooked meat: Especially pork.
Travel or residence history in endemic areas: Southeast Asia, India, Central and South America, Africa.
Family history of parasitic infection: Risk of household transmission.
QCan vegetarians still get cysticercosis?
A
The route of infection is not limited to pork consumption. Infection can also occur through ingestion of water, vegetables, or fruits contaminated with eggs. Therefore, even strict vegetarians are at risk of infection in endemic areas.
Complete blood count (CBC): May show leukocytosis with eosinophilia.
Serological tests: The CDC recommends enzyme-linked immunoelectrotransfer blot (EITB). Commercial ELISA tests are also available but have lower sensitivity.
Cerebrospinal fluid analysis: Performed together with imaging in patients with new-onset seizures due to NCC.
Inexpensive, no radiation, useful for treatment monitoring
CT
Low-density mass + central high-density area (scolex)
Excellent for detecting calcified lesions
MRI
Low-signal cyst + high-signal scolex
Most useful for NCC evaluation. Higher scolex detection rate than CT
Ultrasound is recommended for initial evaluation. Repeated examinations every two weeks are useful for assessing treatment response1). In a study of 161 cases, MRI was shown to be superior to CT in detecting the scolex1). When the cysticerci die, contrast enhancement may be present but the scolex may not be identifiable.
Orbital cysticercosis: Idiopathic orbital myositis, compressive optic neuropathy due to tumor or metastasis, muscle abscess, hematoma, hydatid cyst
NCC: Central nervous system lesions such as abscesses, tumors, etc.
Intraocular cysticercosis: There is a report of a 4-year-old case presenting with imaging findings similar to retinoblastoma, which was later identified as cysticercosis after enucleation. It should be included in the differential diagnosis for intraocular masses in children.
Standard treatment for orbital cysticercosis and NCC is as follows:
Albendazole: 15 mg/kg orally for 4 weeks. It is more effective than praziquantel, especially for large subarachnoid cysticerci.
Corticosteroids: Administer starting at 1.5 mg/kg with gradual tapering. Concomitant use is essential to suppress the inflammatory reaction caused by the death of cysticerci due to antiparasitic drugs.
If scolex cannot be confirmed or ELISA is negative: Oral administration of steroids alone is recommended.
Recurrent cases: Re-administer albendazole and steroids.
Surgical intervention is performed according to the site of infection.
Subconjunctival or eyelid cysticerci: Surgical removal is recommended.
Intravitreal and subretinal cysticerci: Consider vitrectomy before starting drug therapy. This is because when the cysticerci die, the cyst contents are released, leading to severe vitreitis, PVR, glaucoma, and cataract.
NCC with hydrocephalus: Perform surgical removal and drug therapy after placement of a ventriculoperitoneal (VP) shunt.
Laser photocoagulation: Not recommended for subretinal or intravitreal cysticerci due to the risk of severe inflammatory reaction.
QCan drug therapy be applied directly to intravitreal cysticerci?
A
If the cysticerci are killed by drugs, the cyst contents are released into the vitreous cavity, causing a severe inflammatory reaction. Because of the risk of leading to PVR, glaucoma, cataract, and phthisis bulbi, surgical removal by vitrectomy should be performed first. For details, see the section on “Standard Treatment.”
When humans ingest eggs of Taenia solium, gastric acid dissolves the protective capsule of the eggs. The released larvae pass through the intestinal wall and travel via the bloodstream to tissues throughout the body. In the ocular region, they are thought to reach the posterior segment via the short ciliary arteries.
The progression after cysticercus parasitism is classified into three stages1).
Vesicular stage: The cysticercus is alive, and the scolex is clearly visible. The surrounding inflammatory reaction is minimal or absent.
Colloid vesicular stage: The larva begins to die, and the integrity of the cyst wall is lost. Release of toxins causes inflammatory changes in the surrounding tissue.
Calcified nodular stage: The larval remnants are absorbed or calcify to form nodules.
In the posterior segment, the cysticercus migrates from the choroidal circulation across the retina into the vitreous cavity. This process can cause retinal tears, leading to rhegmatogenous retinal detachment. Exudative retinal detachment occurs due to the inflammatory reaction associated with the presence of the cysticercus.
The route of entry into the anterior chamber is still debated, but one theory suggests it occurs via the anterior chamber angle.
The inflammatory reaction upon parasite death is the main cause of ocular complications, and controlling this reaction is key to treatment strategy.
Soman et al. (2021) reported a case of left superior rectus muscle cysticercosis in a 25-year-old woman who had been treated conservatively for recurrent cellulitis for 2 years. Ultrasound B-scan identified the cysticercus and scolex, and MRI confirmed the diagnosis. Symptoms completely resolved after 4 weeks of albendazole 15 mg/kg. No NCC was observed1).
Secondary glaucoma: due to anterior chamber involvement or inflammation.
The prognosis is best for patients who start treatment early and whose imaging findings normalize after the initial infection.
In patients who develop seizures due to NCC, the seizure recurrence rate reaches 49% at 4 years and 68% at 6 years. Long-term management with antiepileptic drugs is often necessary.
In some US states, cysticercosis is reportable to health authorities.
Soman N, Khandelwal R, Maheshwari S. Case of Orbital Cysticercosis Presenting as Recurrent Cellulitis Diagnosed on Multi-Modality Imaging. Cureus. 2021;13(9):e18242.
Pujari A, Bhaskaran K, Modaboyina S, Das D, Saluja G, Samdani A, et al. Cysticercosis in ophthalmology. Surv Ophthalmol. 2022;67(2):544-569. PMID: 34339720.