Opsoclonus-myoclonus syndrome (OMS) is a rare, heterogeneous neurological syndrome first reported by Marcel Kinsbourne in 1962. It is also known as Kinsbourne syndrome or dancing eyes syndrome.
Opsoclonus-myoclonus syndrome is an autoimmune disease characterized mainly by opsoclonus, myoclonus, cerebellar ataxia, cognitive impairment, and behavioral and sleep disorders.
Epidemiology
Annual incidence: 1 in 5 million people
Prevalence: approximately 1 in 1 million people worldwide
In children, incidence is 0.18 per million per year, with a mean age of onset of 1.5 years9)
Typical age of onset in children: 1 to 3 years (12 to 36 months)
In adults, onset occurs across a wide age range from adolescence to the 80s
No clear familial, genetic, sex, or ethnic predisposition
QHow rare is opsoclonus-myoclonus syndrome?
A
The annual incidence is 1 in 5 million, and the prevalence is 1 in 1 million, making it an extremely rare disease. It occurs in both children and adults, but onset in adults is estimated to be even rarer4).
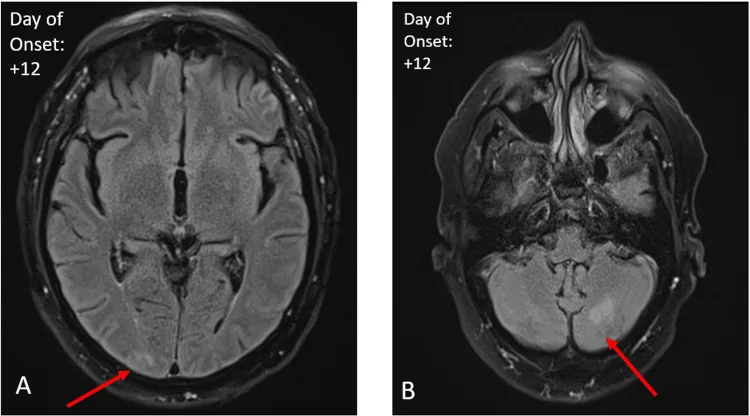
Yang JC, et al. Unique Magnetic Resonance Imaging Findings in Opsoclonus-Myoclonus Syndrome Secondary to the West Nile Virus. Cureus. 2024. Figure 2. PMCID: PMC11426305. License: CC BY.
FLAIR (fluid-attenuated inversion recovery) MRI images; arrows in A and B indicate abnormal signals. These correspond to brain lesions discussed in the section “2. Main Symptoms and Clinical Findings.”
Four diagnostic features of OMS are listed: ① opsoclonus, ② ataxia and/or myoclonus, ③ behavioral changes or sleep disturbances, and ④ diagnosis of neuroblastoma if paraneoplastic.
Opsoclonus
A type of saccadic intrusion, characterized by bursts of multidirectional, irregular, spontaneous conjugate saccades without intersaccadic intervals. It disrupts fixation and is observed as high-frequency, high-amplitude chaotic eye movements in all directions. It may not be present at initial evaluation and can appear several weeks after the onset of motor symptoms.
Myoclonus
It has diverse characteristics and can affect any part of the body. It worsens with emotional stress or attempted movement. In COVID-19-related cases, generalized stimulus-sensitive myoclonus and action myoclonus have been reported1).
Cerebellar ataxia
Presents with gait disturbance, truncal ataxia, and wide-based gait.
Others
May be accompanied by dysarthria, limb and jaw tremor, and voice tremor1, 5, 8).
The table below shows the differential points between opsoclonus and similar abnormal eye movements.
QHow do you differentiate opsoclonus from nystagmus?
A
Nystagmus has a slow phase (slow movement), but opsoclonus does not. Ocular flutter also lacks a slow phase and consists of rapid horizontal eye movements only, whereas opsoclonus involves multiple directions. Square-wave jerks are rapid saccadic movements but differ in that they maintain normal saccadic intervals.
The exact etiology is unknown, but autoimmune inflammation due to infectious or paraneoplastic processes is a leading hypothesis. Cellular and humoral immune mechanisms are involved, and most patients are seronegative for known anti-neuronal antibodies.
The etiology is broadly classified into three categories.
Paraneoplastic
Children: Approximately 50% of OMS patients have an underlying neuroblastoma. About 2% of children with neuroblastoma develop OMS.
Adults: 20–40% of OMS cases are paraneoplastic. Small cell lung cancer (SCLC) is the most common, followed by breast adenocarcinoma8). In women under 30, ovarian teratoma is associated6).
Associated antibodies: Anti-Ri (ANNA-2) is the most typical2). Anti-Hu, anti-Ma, etc. Antibody-negative paraneoplastic OMS also exists7).
Post-infectious/Infection-associated
Main associated pathogens: Lyme disease, EBV, HIV (immune reconstitution syndrome), Mycoplasma pneumoniae, rotavirus.
COVID-19 related: Onset occurs 2 days to 3 weeks after respiratory symptoms1).
West Nile virus-related: There are case reports of improvement with IVIG3).
Post-vaccination: Onset after varicella, measles, and DPT vaccines has been reported.
Toxic/metabolic
It can also occur with phenytoin overdose, hyperosmolar nonketotic diabetic coma, cocaine intoxication, etc.
QAre there differences in causes between children and adults?
A
In children, about 50% have an underlying neuroblastoma, so all pediatric OMS cases require evaluation for neuroblastoma9). In adults, 20–40% of OMS cases are paraneoplastic, with small cell lung cancer and breast cancer being common associated tumors. Onset after infection can occur at any age.
OMS is a clinical diagnosis based on clinical findings, and there are no definitive tests or biomarkers. Diagnostic delay is common, with a median time from symptom onset to diagnosis of 11 weeks 4).
For differentiation from nystagmus, ocular flutter, and square-wave jerks, refer to the “Clinical Findings” section. Other differential diagnoses include vestibular neuritis, benign paroxysmal positional vertigo, stroke, brain tumor, autoimmune encephalitis, multiple sclerosis, and oculomotor apraxia 4, 7). Oculomotor apraxia is a disorder of saccadic eye movements and is distinguished from opsoclonus by the characteristic head thrusts during gaze shifts to new targets.
The purpose is to exclude primary CNS disease. MRI is normal in many OMS cases. Some cases show T2-FLAIR hyperintensities (cerebellum, temporal lobes) 3, 2), and cerebellar atrophy may be observed in the chronic phase 9).
Cerebrospinal Fluid (CSF) Analysis
Used to exclude CNS diseases. Normal to mildly abnormal in many cases. Some cases show positive oligoclonal bands and mildly elevated protein 2, 4). Expansion of CD19+ B cells in CSF (up to 29%) is being studied as a candidate disease activity biomarker4).
Malignancy screening
Children: Consider evaluation for neuroblastoma in all cases.
Adults: Perform CT, PET-CT 7, 8). If no tumor is found, follow up every 6 months for up to 4 years 2).
Anti-neuronal antibody panel
Search for anti-Ri (ANNA-2), anti-Hu, anti-Yo, anti-Ma, anti-NMDA receptor, etc. However, many patients are antibody-negative.
PNS-Care scoring system (2021 International Panel) considers clinical phenotype, antibody type, presence of cancer, and follow-up duration, classifying into definite (>8 points), probable (6–7 points), and possible (4–5 points) 7).
The mainstay of treatment is immunomodulatory therapy. In paraneoplastic cases, tumor-targeted therapy is essential and should be performed concurrently with immunomodulatory therapy. Early treatment is important because delayed diagnosis is associated with worse neurological, psychological, and behavioral outcomes.
Intravenous methylprednisolone pulse therapy (1 g/day for 3–5 days) is the standard protocol 2, 6, 7).
ACTH (Adrenocorticotropic Hormone)
It is positioned as a standard treatment for children and adults.
IVIG (Intravenous Immunoglobulin)
A total dose of 2 g/kg divided over 3–5 days is common 1, 6). Reports include improvement starting after 1 week and complete recovery after 4 weeks in a COVID-19-related case 1), and improvement after 5 days of administration in a West Nile virus-related case 3).
It is added for cases where steroids and IVIG are insufficient. In ovarian teratoma-associated OMS, a report describes no recurrence for 30 months after two doses of 1 g, followed by additional doses at 6 and 12 months 6). It has been suggested that combination immunosuppression may be more effective than single-agent therapy.
Tumor-targeted therapy (surgery, chemotherapy, radiotherapy) is essential. Tumor resection does not always lead to neurological improvement, and there are reports of OMS onset one month after resection6). In small cell lung cancer, carboplatin plus etoposide chemotherapy8) has been reported to improve symptoms, and in breast cancer, neoadjuvant chemotherapy plus rituximab has shown improvement7).
QHow long does treatment need to continue?
A
The treatment duration varies depending on etiology, severity, and treatment response. While some cases improve within weeks to months with IVIG3, 4), long-term immunosuppressive therapy such as rituximab may be necessary to prevent recurrence6). Paraneoplastic OMS tends to be more severe and treatment-resistant than idiopathic OMS8).
There are two main theories regarding the pathogenesis of OMS: the brainstem theory and the cerebellar theory.
Brainstem Theory
Abnormality of saccadic burst neurons: Burst neurons are normally under sustained inhibition from omnipause neurons.
Mechanism: Increased neuronal excitability of burst neurons due to altered membrane properties, or reduced inhibition from omnipause neurons, leads to ocular oscillations.
Cerebellar Theory
Disinhibition of the caudal fastigial nucleus: Dysfunctional Purkinje cells fail to inhibit the fastigial nucleus.
Pathogenesis: The fastigial nucleus enhances inhibition of omnipause neurons → saccadic burst neurons oscillate freely → opsoclonus. Supporting findings include gliosis and inflammation of the cerebellar vermis, increased cerebellar blood flow in the acute phase, and hypoperfusion and atrophy in the chronic phase9).
Opsoclonus itself usually resolves regardless of treatment. However, relapse after remission is possible, and abnormalities in smooth pursuit eye movements may persist long after opsoclonus disappears. Behavioral and psychomotor disorders remain in 60–80% of patients, and long-term neurological prognosis is often poor.
Paraneoplastic OMS tends to be more severe and less responsive to treatment than idiopathic OMS8)
Post-infectious/idiopathic OMS responds well to immunosuppressive therapy and has a relatively favorable course8)
Adult idiopathic OMS usually has a benign outcome4)
7. Latest Research and Future Perspectives (Investigational Reports)
In a 7-case series by Emamikhah et al. (2021), OMS developed 2 days to 3 weeks after COVID-19 respiratory symptoms and improved with IVIG1). In an adult review, about one-third had influenza-like prodrome, and 40% had elevated IgG index or oligoclonal bands.
OMS after COVID-19 is increasingly recognized as an independent immune-mediated parainfectious syndrome without encephalopathy.
Yang et al. (2024) reported a course of normal initial MRI, followed by T2-FLAIR hyperintensity at 10 days, and complete resolution at 4 months 3). This suggests a specific time window may exist between symptom onset and MRI abnormality detection.
The anti-Ri syndrome, previously considered OMS plus ataxia, is being redefined as a more complex multisystem disorder.
Freydl et al. (2024) proposed a triad of gait disturbance, ocular movement disorder, and jaw dystonia as a characteristic syndrome 2). About 80% of PNS patients are diagnosed with a tumor within 4 to 6 months after symptom diagnosis.
In the Pranzatelli study (cited in Lawrence 2025), expansion of CD19+ B cells in the CSF has been proposed as a candidate disease activity biomarker for OMS 4). Standardization has not yet been achieved.
Late-onset OMS, triggered by immune activation due to antigen exposure after tumor resection, has been recognized 6). Additionally, immune checkpoint inhibitors have been reported to potentially induce or exacerbate OMS and brainstem encephalitis as immune-related adverse effects 5), and in cases of PD-L1-high tumors, avoidance of such agents may be considered.
Emamikhah M, Babadi M, Mehrabani M, Jalili M, Pouranian M, Daraie P, et al. Opsoclonus-myoclonus syndrome, a post-infectious neurologic complication of COVID-19: case series and review of literature. Journal of neurovirology. 2021;27(1):26-34. doi:10.1007/s13365-020-00941-1. PMID:33492608; PMCID:PMC7831695.
Elisabeth Freydl, Alexander Tinchon, Katrin Blauensteiner, Stefan Oberndorfer. Anti-Ri paraneoplastic neurological syndrome presenting with bilateral cranial nerve VI palsy and jaw dystonia-a distinctive syndrome within the anti-Ri spectrum? : Case report and literature review. Wien Med Wochenschr. 2024;174(1-2):16-21. doi:10.1007/s10354-023-01006-8.
Yang JC, Zekavaty S, Rossi RD, Mahmoud SY. Unique Magnetic Resonance Imaging Findings in Opsoclonus-Myoclonus Syndrome Secondary to the West Nile Virus. Cureus. 2024;16(8):e67932. doi:10.7759/cureus.67932.
Lawrence JS. Challenges in Diagnosing Opsoclonus-Myoclonus Syndrome in Adults. Cureus. 2025;17(5):e84780. doi:10.7759/cureus.84780. PMID:40557009; PMCID:PMC12186758.
Costa PA, Costa BMLA, Rozenbaum G, Barreto-Coelho P. Anti-Ma paraneoplastic opsoclonus-myoclonus syndrome. BMJ case reports. 2021;14(5). doi:10.1136/bcr-2021-243136. PMID:33975854; PMCID:PMC8117984.
Jones AA, Chen T. Delayed Opsoclonus-Myoclonus Syndrome After Ovarian Teratoma Resection. Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society. 2022;42(1):e450-e451. doi:10.1097/WNO.0000000000001384. PMID:34417773; PMCID:PMC8834143.
Soares R, Mittapalli A, Ramakrishnan M, Farooq U. Breast Cancer Presenting As Onconeural Antibody Negative Opsoclonus-Myoclonus Syndrome. Cureus. 2022;14(8):e28417. doi:10.7759/cureus.28417. PMID:36046059; PMCID:PMC9416628.
Moreira I, Vilas-Boas I, Cassiano Neves M. Paraneoplastic Opsoclonus-Myoclonus Syndrome as a Rare Presentation of Small-Cell Lung Cancer. Cureus. 2022;14(11):e32066. doi:10.7759/cureus.32066. PMID:36600862; PMCID:PMC9800942.
Takenaka J, Hirata K, Watanabe S, Shiraishi H, Kudo K. Neuroblastoma-related severe hypoperfusion in the cerebellum of an infant: A case of opsoclonus-myoclonus syndrome. Asia Oceania journal of nuclear medicine & biology. 2023;11(1):93-96. doi:10.22038/AOJNMB.2022.65833.1459. PMID:36619191; PMCID:PMC9803626.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.