Cancer-associated retinopathy (CAR) is an autoimmune retinal degenerative disease that occurs in association with malignant tumors. It is classified as an ocular manifestation of paraneoplastic syndrome1).
The disease concept and autoimmune mechanism were established in the 1970s–1980s. Tumor cells ectopically express antigens that cross-react with retinal proteins, leading to the production of autoantibodies that damage photoreceptor cells.
In the classification of autoimmune retinopathy (AIR), it is broadly divided into tumor-associated AIR and non-tumor-associated AIR (npAIR). Tumor-associated AIR includes CAR and melanoma-associated retinopathy (MAR) 1).
The most frequent causative tumor is small cell lung cancer (SCLC), followed by gastrointestinal cancer, gynecological cancer, breast cancer, renal cancer, pancreatic cancer, and lymphoma. The age of onset ranges from 40 to 85 years, with no clear sex difference. In a series of 209 cases by Adamus et al., a female predominance was reported.
Ocular immune-related adverse events associated with ICI have been reported, and differentiation from CAR/MAR-like retinal symptoms may be problematic 3).
QCan cancer be found after eye symptoms appear?
A
In many cases, ocular symptoms precede the diagnosis of cancer. Although it is a relatively rare disease, an ophthalmological diagnosis can lead to the discovery of systemic cancer. In patients aged 50 years or older with fundus findings similar to retinitis pigmentosa (RP) and no family history, CAR should be suspected and systemic evaluation should be considered 4).
Subjective symptoms of CAR are characterized by subacute, bilateral (often asymmetric) painless vision loss, progressing over weeks to months.
Photopsia and photophobia: These symptoms often appear early.
Night blindness and visual field constriction: In rod-dominant type, ring scotoma and visual field constriction are predominant.
Central scotoma and color vision abnormality: In cone-dominant type, photophobia, central scotoma, and color vision disturbance are prominent.
Symptom characteristics vary depending on the causative antibody. Anti-recoverin antibody-positive cases often present with rapid and severe vision loss, forming paracentral to equatorial scotomas. Anti-enolase antibody-positive cases tend to show relatively slow, asymmetric central vision loss.
A representative case is reported as follows1).
Bordin et al. (2023) Case 1: 58-year-old woman. After lobectomy for a right lung tumor, she reported progressive vision loss, visual field narrowing, and bilateral scotomas. Best corrected visual acuity was 20/401).
Case 2: 66-year-old man. He had a history of nephrectomy for a renal tumor 1.5 years ago and presented with progressive painless vision loss. Right eye 20/200, left eye hand motion.
In cases of rapid vision loss during ICI administration, drug-related ocular inflammation, tumor-associated AIR, and metastatic lesions should be evaluated concurrently3).
Rod-dominant type
Main symptoms: Night blindness, visual field narrowing, ring scotoma
Representative antibody: Anti-recoverin antibody
Progression speed: Rapid (weeks to months)
Features: Rapid severe vision loss. Paracentral to equatorial scotomas are typical.
Cone-dominant type
Main symptoms: Photophobia, central scotoma, color vision abnormality
Tumor cells ectopically express retinal proteins that normally have immune privilege, leading to the production of autoantibodies against them. Molecular mimicry plays an important role1). The main autoantibodies are as follows.
Anti-recoverin antibody: A representative CAR-associated antibody. It can be positive even without malignancy 2, 4).
Anti-α-enolase antibody: Relatively common.
Others: Many autoantibodies have been reported, including anti-carbonic anhydrase II (CAII), anti-transducin β, anti-TULP1, anti-arrestin, and anti-GAPDH.
ICIs release immune checkpoints and can underlie autoimmune ocular adverse events. When retinal symptoms occur, it is important to differentiate between drug-related ocular adverse events and tumor-associated AIR 3).
Small cell lung cancer is the most common, followed by breast cancer, gastrointestinal cancer, gynecologic cancer, kidney cancer, pancreatic cancer, and lymphoma. In MAR, malignant melanoma is the main causative tumor.
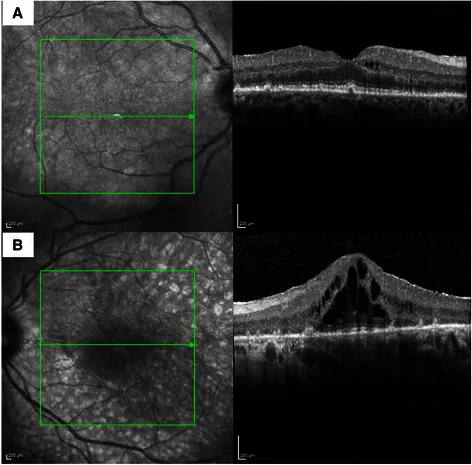
Maria Pefkianaki; Rupesh Agrawal; Parul Desai; Carlos Pavesio; Mandeep S Sagoo. Bilateral Diffuse Uveal Melanocytic Proliferation (BDUMP) associated with B-cell lymphoma: report of a rare case. BMC Cancer. 2015 Jan 30; 15:23 Figure 4. PMCID: PMC4320603. License: CC BY.
Spectral domain OCT (Heidelberg) scans of right (A) and left (B) eyes showing presence of retinal pigment epithelial disturbances with excrescences at level of retinal pigment epithelium and presence of subretinal fluid in the left eye.
There are no established diagnostic criteria; diagnosis is made by combining clinical findings, electrophysiological tests, autoantibody tests, and systemic cancer screening.
This is the most important test for diagnosis. It is also essential for differentiating CAR and MAR.
CAR: Both a-wave and b-wave are reduced in dark adaptation (rod system) and light adaptation (cone system).
MAR: Negative electroretinogram (a-wave is normal or nearly normal but b-wave is markedly reduced) is characteristic, reflecting bipolar cell dysfunction.
In a report of a 2-year-old child with APECED (autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy), the electroretinogram was non-recordable, and OCT confirmed loss of ELM and EZ2).
Retinal autoantibodies can be positive in healthy individuals and npAIR, so they cannot be used alone for a definitive diagnosis. Since antibody titers fluctuate, measurement at least three times is recommended.
For systemic cancer workup, consider chest X-ray, CT, blood tests, abdominal CT, PET, colonoscopy, and evaluation of the breast and urogenital organs. In patients aged 50 years or older with fundus findings similar to RP and no family history, systemic investigation should be considered 4).
The following table shows the main differentiating points between CAR and MAR.
Feature
CAR
MAR
Damaged cells
Photoreceptor cells
Bipolar cells
Electroretinogram findings
Decreased a-wave and b-wave
Negative electroretinogram
Causative tumor
Various, e.g., lung cancer
Malignant melanoma
QCan CAR be diagnosed if anti-retinal autoantibodies are positive?
A
Positive anti-retinal autoantibodies alone do not confirm a diagnosis of CAR. They can also be positive in healthy individuals and npAIR, and antibody titers fluctuate. It is necessary to comprehensively evaluate electrophysiological and morphological findings such as electroretinography, OCT, and FAF, as well as the presence or absence of systemic malignancy.
QHow to differentiate between CAR and MAR?
A
Electroretinogram findings are the most important differentiating feature. In CAR, both rod and cone systems show reduced a-wave and b-wave, whereas in MAR, a negative electroretinogram (normal a-wave, markedly reduced b-wave) is observed. In MAR, malignant melanoma is often the causative tumor, while in CAR, small cell lung cancer is more common. The affected cells also differ: CAR affects photoreceptors, while MAR affects bipolar cells.
There are no established treatment guidelines. The goal of treatment is not complete recovery but stabilization of function, with the main focus on suppressing progression 1).
Systemic steroids: There are reports of improvement, but due to the risk of suppressing cancer immunity, cautious administration is required.
Immunosuppressive drugs: Cyclosporine, azathioprine, alemtuzumab, etc., are used.
Rituximab (anti-CD20 antibody): In a report of 16 AIR cases (including 6 CAR), 77% of eyes showed stabilization or improvement with combination therapy.
IVIG (intravenous immunoglobulin): Used to neutralize autoantibodies. Some reports of efficacy exist.
Plasma exchange: Performed to remove autoantibodies.
Local therapy: Dexamethasone intravitreal implant (Ozurdex)
In a 2023 report by Bordin et al., for cases where oral steroids and sub-Tenon steroid injections were ineffective and systemic immunosuppressants were intolerable, Ozurdex administered every 6 months resulted in functional stabilization1).
Ozurdex is thought to control local inflammation through sustained drug release over 3–4 months and contribute to restoration of the blood-retinal barrier (BRB). Monitoring of anti-recoverin antibody titers also showed a decrease after Ozurdex administration1).
Anti-IL-6 receptor antibodies (tocilizumab, sarilumab) have been reported for use in npAIR with refractory cystoid macular edema1).
Even after resection, chemotherapy, or radiotherapy of the primary tumor, visual improvement is often not achieved due to autoantibodies already circulating in the body 1). Tumor treatment is performed as systemic management, but it is difficult to expect improvement in ocular lesions with tumor treatment alone.
In APECED-related retinal cases, it has been reported that retinal degeneration progressed despite immunosuppressive therapy2).
QWill eye symptoms improve if the cancer is treated?
A
Even if the primary tumor is treated, autoantibodies already produced and circulating in the body are difficult to eliminate, so visual recovery is often not achieved 1). Tumor treatment is essential for systemic management, but its effect on ocular lesions is limited. The goal of treatment should be stabilization of visual function.
When tumor cells ectopically express proteins that are normally expressed only in immune-privileged sites (retina), the immune system recognizes them and produces autoantibodies. This molecular mimicry initiates retinal damage 1).
Anti-recoverin antibodies are thought to enter cells, impair calcium homeostasis, and induce apoptosis. In CAR, both rod and cone photoreceptors are simultaneously damaged 4).
MAR has a different mechanism and involves autoantibodies against the bipolar cell membrane protein (TRPM1). The difference in affected cells manifests as the aforementioned differences in electroretinogram findings (CAR shows decreased a+b waves, MAR shows negative ERG).
ICIs enhance T-cell responses and can induce autoimmune inflammation. In ophthalmology, adverse events such as uveitis, ocular inflammation, and dry eye have been reported 3).
If retinal symptoms are observed during ICI use, differentiate between drug-related ocular adverse events, paraneoplastic autoimmune retinopathy, and tumor metastasis based on clinical course and imaging studies.
7. Latest Research and Future Perspectives (Reports Under Investigation)
Ozurdex is attracting attention as a local treatment option for cases where systemic immunosuppressive therapy is difficult. In a case report by Bordin et al. (2023), repeated administration every 6 months resulted in functional stabilization and a decrease in anti-recoverin antibody titers 1). Combining post-administration autoantibody monitoring may enable evaluation of treatment response.
With the widespread use of ICIs, there is a growing need to differentiate drug-related ocular adverse events from CAR/MAR 3). Establishing early diagnosis and appropriate intervention protocols remains a future challenge.
Anti-IL-6 receptor antibodies such as tocilizumab and sarilumab have been used for AIR with refractory cystoid macular edema, and their application to CAR is also being considered 1).
Calcium channel blockers have been shown to be effective in a CAR rat model, and future research is expected as an intervention for calcium homeostasis impairment caused by anti-recoverin antibodies.
In APECED caused by AIRE gene mutations, cases of autoimmune retinopathy developing from early childhood have been reported 2). Sakaguchi et al. (2021) reported that electroretinography became non-recordable at age 2, suggesting the importance of early intervention, but effective treatment has not yet been established 2).
Bordin FL, et al. Intravitreal Dexamethasone Implant in Autoimmune Retinopathy. Case Rep Ophthalmol Med. 2023;2023:5670538.
Sakaguchi H, Mizuochi T, Haruta M, Takase R, Yoshida S, Yamashita Y, Nishikomori R. AIRE gene mutation presenting at age 2 years with autoimmune retinopathy and steroid-responsive acute liver failure: a case report and literature review. Front Immunol. 2021;12:687280. doi:10.3389/fimmu.2021.687280.
Fang T, Maberley DA, Etminan M. Ocular adverse events with immune checkpoint inhibitors. J Curr Ophthalmol. 2019;31(3):319-322. doi:10.1016/j.joco.2019.05.002.
Brossard-Barbosa N, Dezard V, Margolin E. Treatment of Cancer-Associated Retinopathy: A Systematic Literature Review. Ophthalmol Retina. 2023 Sep;7(9):819-828. doi:10.1016/j.oret.2023.05.002. PMID:37160190.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.