Anterior chamber washout is a procedure in which pathologically accumulated substances in the anterior chamber are flushed out with irrigation fluid. Pathological substances targeted for washout include blood, pus, inflammatory mediators, chemicals, and ophthalmic viscosurgical devices (OVDs). Anterior chamber washout is not an independent disease but is positioned as a therapeutic procedure performed for various anterior segment diseases and postoperative complications.
The anterior chamber is a closed space of approximately 0.2 mL, with the only substantial outflow route being the aqueous humor drainage pathway through the trabecular meshwork. In conditions such as endophthalmitis, hyphema, and chemical burns where pathological substances accumulate rapidly, natural drainage is limited, and early mechanical removal directly protects intraocular tissues such as the corneal endothelium, iris, and lens.
Removal of intraocular chemical substances and reduction of inflammation
In addition to the above five diseases, anterior chamber irrigation is also performed in the following conditions.
Elevated intraocular pressure due to retained OVD after cataract surgery: Removes viscoelastic material that causes transient postoperative elevated intraocular pressure.
UGH syndrome: Performed adjunctively for iris chafing, pigment dispersion, and chronic hyphema due to IOL malposition.
Hyphema after MIGS or trabeculotomy: Indicated when postoperative bleeding persists.
Meta-analyses have shown that intraoperative intracameral antibiotic administration reduces the risk of postoperative endophthalmitis1), and the importance of intraoperative antibiotic administration is recognized from a prophylactic perspective of anterior chamber irrigation.
QIn what cases is anterior chamber irrigation necessary?
A
The main indications are conditions where pathological substances accumulate in the anterior chamber, such as endophthalmitis, hyphema, and chemical burns. It is also indicated for elevated intraocular pressure due to retained viscoelastic material after cataract surgery, and for non-infectious anterior segment inflammation called TASS. Surgical irrigation is chosen when conservative treatment fails to improve the condition, or when prevention of irreversible complications such as corneal blood staining is necessary.
2. Symptoms and clinical findings requiring anterior chamber irrigation
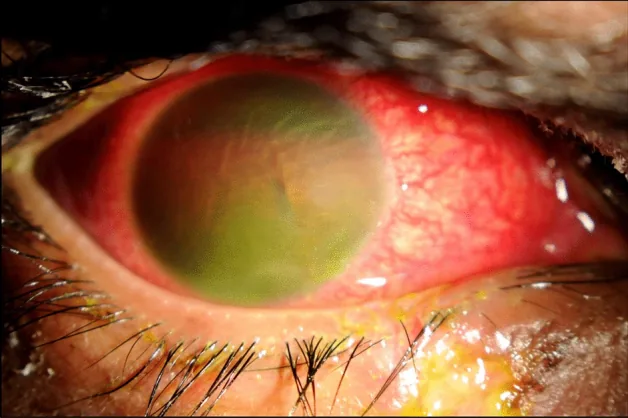
AlGhadeer H, et al. Fireworks ocular injury in Saudi children: profile and management outcomes. Sci Rep. 2022. Figure 1. PMCID: PMC8993825. License: CC BY.
Slit-lamp photograph showing the anterior chamber filled with blood due to severe traumatic hyphema, making observation of the iris and pupil difficult. This is a representative example of symptoms and clinical findings requiring anterior chamber irrigation.
The main subjective symptoms that occur depending on the condition requiring anterior chamber irrigation are shown below.
Endophthalmitis (infectious): Rapid vision loss, eye pain, redness, and increased discharge within a few days after surgery. Rapid progression of symptoms is characteristic.
TASS (noninfectious anterior segment inflammation): Decreased vision and conjunctival injection within 1–2 days after surgery. Onset is earlier than infectious endophthalmitis, and eye pain is often relatively mild8).
Hyphema: Decreased vision, eye pain, conjunctival injection, photophobia. Visual loss worsens in proportion to the amount of bleeding.
Chemical burn: Severe eye pain, conjunctival injection, decreased vision. Alkali burns penetrate into the anterior chamber rapidly.
Residual OVD: Eye pain and headache within a few hours after cataract surgery (symptoms mainly due to elevated intraocular pressure).
Slit-lamp examination of the anterior chamber determines the need for and urgency of irrigation.
Moderate
Hypopyon: White to yellow fluid level in the inferior anterior chamber. Seen in endophthalmitis and TASS.
Hyphema with fluid level: Formation of a blood level in the anterior chamber. Corresponds to Grade I–II.
Fibrin deposition: Reticular to membranous deposits appear in the anterior chamber.
Severe
Total hypopyon/total hyphema: The entire anterior chamber is filled with inflammatory material or blood. Corresponds to Grade III–IV.
Mutton-fat keratic precipitates: Large inflammatory cell deposits on the corneal endothelium. Suggests severe endophthalmitis.
Corneal edema/opacity: Reflects sustained high intraocular pressure or corneal endothelial damage.
Inability to visualize the fundus: Ultrasound examination is necessary to determine the need for vitrectomy.
QIf vision suddenly decreases after cataract surgery, is endophthalmitis a possibility?
A
Acute postoperative vision loss is an important sign of endophthalmitis. Onset within 1–2 days after surgery suggests TASS (non-infectious), while onset from several days to one week postoperatively strongly suggests infectious endophthalmitis1). TASS primarily presents with hyperemia and vision loss, often with mild eye pain, whereas infectious endophthalmitis is accompanied by eye pain, discharge, and hypopyon. Prompt ophthalmologic evaluation is essential in either case.
Systemic factors: Immunocompromised state and diabetes
Surgical factors: Surgeon experience, prolonged surgery time, inferior incision (higher risk of contamination from eyelid secretions)
Causative organisms: The most common is Staphylococcus epidermidis (coagulase-negative Staphylococcus), accounting for approximately 60–70% of all cases7)
Blunt trauma: Most common cause. Compressive force to the eye ruptures blood vessels of the iris and ciliary body.
Iatrogenic: After cataract surgery, MIGS, or UGH syndrome. When an IOL is fixated outside the capsule or asymmetrically, the haptic rubs against the iris, causing iris pigment to clog the trabecular meshwork and leading to pigmentary glaucoma. Significant iris damage may be accompanied by iridocyclitis and hyphema (UGH syndrome).
Prolonged hyphema and elevated intraocular pressure are the main causes.
In patients with sickle cell disease, red blood cells sickle in the hypoxic environment of the anterior chamber, leading to severe intraocular pressure elevation even with small amounts of bleeding. Early surgical washout is important.
Alkalis (such as lime and strong alkaline detergents) are fat-soluble, so they penetrate the full thickness of the cornea into the anterior chamber, causing rapid pH changes. Acid burns form a protein coagulation layer in the corneal stroma, limiting penetration into the anterior chamber, but strong acids can reach the anterior chamber.
The following examinations are performed in combination to determine the indication for anterior chamber irrigation.
Slit-lamp microscopy: Evaluates hypopyon, hemorrhage, fibrin, and OVD retention in the anterior chamber. Record the height, color, and extent of hypopyon.
Intraocular pressure measurement: OVD retention often causes a rapid rise in intraocular pressure within hours after surgery. In hyphema, intraocular pressure rises due to trabecular meshwork obstruction by red blood cells.
Visual acuity testing: Record visual acuity changes at initial visit and during follow-up.
Fundus examination: In endophthalmitis, the presence of vitreous opacity is important and directly influences the decision to perform anterior chamber irrigation alone or add vitrectomy.
Aqueous humor collection and bacterial culture: If endophthalmitis is suspected, collect 0.2 mL of aqueous humor from the side port using a 27G needle and submit for bacterial culture and drug sensitivity testing.
Sickle cell screening: Perform for patients with hyphema who are at risk (African or Mediterranean descent).
If vitreous opacity is severe → prioritize emergency vitrectomy
QHow long does hyphema last before surgery is needed?
A
In healthy individuals, anterior chamber washout is indicated when intraocular pressure is 50 mmHg or higher for 5 days or more, or 35 mmHg or higher for 7 days or more11). If signs of corneal blood staining are present, early surgery should be considered regardless of intraocular pressure level. In patients with sickle cell disease, the criteria are stricter: intervention should be considered if pressure is 25 mmHg or higher for more than 24 hours. In children, more aggressive decision-making is required due to the risk of amblyopia from visual deprivation.
This is indicated when inflammation is confined to the anterior chamber and vitreous opacity is mild. Along with anterior chamber irrigation, the following antibiotics are injected into the anterior chamber and vitreous cavity.
Vancomycin: 1 mg/0.1 mL (covers gram-positive bacteria)
Ceftazidime: 2.25 mg/0.1 mL (covers gram-negative bacteria)
If vitreous opacity is extensive, emergency vitrectomy is performed. According to the EndophthalmitisVitrectomy Study (EVS), in acute postoperative endophthalmitis with initial visual acuity of hand motion (HM) or better, tap and inject and immediate vitrectomy showed equivalent visual outcomes. However, for eyes with initial visual acuity of light perception (LP) or worse, immediate vitrectomy was significantly superior3).
If the blood clot is large or hardened, it is removed with forceps or excised and aspirated with a vitreous cutter.
Timing of surgery: Approximately 4 days after injury is appropriate. This corresponds to the time when the risk of rebleeding decreases and the blood clot has separated from ocular tissues9, 11).
TASS is a non-infectious anterior segment inflammation that develops within 1–2 days after surgery, and differentiation from infectious endophthalmitis is important. The timing of onset, degree of eye pain, and culture results of the anterior chamber fluid should be comprehensively evaluated 8). In many cases, anterior chamber irrigation and aggressive steroid eye drops rapidly reduce inflammation.
Rest and head elevation: After anterior chamber hemorrhage washout, elevate the head to 30–45 degrees to prevent rebleeding 10).
QCan anterior chamber irrigation be performed as a day procedure?
A
If performed as an outpatient procedure (two-site puncture method), it may be possible as a day procedure. Irrigation using an I/A device in the operating room can also be done as a day procedure for mild cases, but for endophthalmitis or severe hyphema, hospitalization is desirable for postoperative infection control and systemic management.
The anterior chamber has the trabecular meshwork and Schlemm’s canal as its only substantial outflow pathway for aqueous humor. When blood, pus, viscoelastic substances, or chemicals accumulate in this space, the outflow mechanism becomes physically and chemically obstructed, leading to a cascade of elevated intraocular pressure and tissue damage.
When high intraocular pressure persists and hyphema is prolonged, the pump function of the corneal endothelium is impaired. Hemoglobin breakdown products (hemin, bilirubin, etc.) gradually deposit in the corneal stroma, causing the cornea to become yellowish-brown to brown and cloudy. Once corneal blood staining develops, there is no effective treatment, and only waiting for absorption is possible. Therefore, from a preventive perspective, early anterior chamber washout is important to prevent the development of corneal blood staining in cases of prolonged hyphema with elevated intraocular pressure.
Intraocular pressure elevation due to retained OVD
Viscoelastic substances (such as sodium hyaluronate) are used in the anterior chamber and capsular bag during surgery. If not sufficiently removed postoperatively, their viscosity can physically obstruct the trabecular meshwork, causing transient postoperative ocular hypertension12). High molecular weight, high viscosity OVDs carry a higher risk of intraocular pressure elevation.
Alkali is fat-soluble and therefore penetrates the full thickness of the cornea, raising the pH in the anterior chamber. pH changes damage the corneal endothelium, iris stroma, and lens epithelium. Alkali dissolves intraocular lipid membranes and causes tissue necrosis, so rapid dilution and removal of alkali from the anterior chamber is important to reduce tissue damage.
When an intraocular lens is fixated outside the capsular bag or becomes asymmetrically fixated, the haptic directly contacts and rubs against the iris. Iris pigment clogs the trabecular meshwork, leading to pigmentary glaucoma. If iris damage is severe, it may be accompanied by iridocyclitis and hyphema (uveitis-glaucoma-hyphema syndrome). If conservative treatment does not improve the condition, IOL exchange or removal is necessary.
Large multicenter studies have shown the efficacy of intracameral cefuroxime (1 mg/0.1 mL) administration during surgery for preventing postoperative endophthalmitis. The risk of endophthalmitis was significantly reduced in the intracameral cefuroxime group, with an odds ratio of 0.26 (95% CI: 0.15–0.45)1). Anterior chamber irrigation is a treatment procedure for postoperative endophthalmitis, but prophylactic intracameral antibiotic administration during surgery is becoming more widespread.
Reduction of Intraoperative Anterior Chamber Bacterial Contamination via Povidone-Iodine Irrigation
The Shimada method, which involves repeated intraoperative irrigation of the ocular surface with 0.25% povidone-iodine solution, has been reported to reduce the rate of anterior chamber bacterial contamination at the end of surgery (p = 0.0017)6). Intraoperative irrigation in addition to conventional preoperative disinfection may contribute to the prevention of postoperative endophthalmitis.
Reevaluation of Systemic Antimicrobial Therapy for Postoperative Endophthalmitis
Recent systematic reviews have pointed out that systemic antibiotics have limited intravitreal penetration in postoperative endophthalmitis5), leading to a reassessment of the role of systemic administration. Local administration into the anterior chamber and vitreous cavity is considered the mainstay of treatment, while systemic administration is thought to play only an adjunctive role.
Bowen RC, Zhou AX, Bondalapati S, et al. Comparative analysis of the safety and efficacy of intracameral cefuroxime, moxifloxacin and vancomycin at the end of cataract surgery: a meta-analysis. Br J Ophthalmol. 2018;102(9):1268-1276. doi:10.1136/bjophthalmol-2017-311051. PMID:29326317; PMCID:PMC6041193.
Miller KM, Oetting TA, Tweeten JP, et al. Cataract in the Adult Eye Preferred Practice Pattern. Ophthalmology. 2022;129(1):P1-P126. doi:10.1016/j.ophtha.2021.10.006. PMID: 34780842.
EndophthalmitisVitrectomy Study Group. Results of the EndophthalmitisVitrectomy Study. A randomized trial of immediate vitrectomy and of intravenous antibiotics for the treatment of postoperative bacterial endophthalmitis. EndophthalmitisVitrectomy Study Group. Arch Ophthalmol. 1995;113(12):1479-96. doi:10.1001/archopht.1995.01100120009001. PMID:7487614.
Wallin T, Parker J, Jin Y, Kefalopoulos G, Olson RJ. Cohort study of 27 cases of endophthalmitis at a single institution. Journal of cataract and refractive surgery. 2005;31(4):735-41. doi:10.1016/j.jcrs.2004.10.057. PMID:15899450.
Brockhaus L, Goldblum D, Eggenschwiler L, Zimmerli S, Marzolini C. Revisiting systemic treatment of bacterial endophthalmitis: a review of intravitreal penetration of systemic antibiotics. Clin Microbiol Infect. 2019;25(11):1364-1369. doi:10.1016/j.cmi.2019.01.017. PMID: 30771529.
Shimada H, Nakashizuka H. Cataract surgery by intraoperative surface irrigation with 0.25% povidone-iodine. J Clin Med. 2021;10(16):3611. doi:10.3390/jcm10163611. PMID: 34441906.
Cutler Peck CM, Brubaker J, Woods SE, Chan E, Mettu P, Cousins SW. Toxic anterior segment syndrome: common causes. J Cataract Refract Surg. 2010;36(7):1073-1080. doi:10.1016/j.jcrs.2010.01.030. PMID: 20610082.
Deutsch TA, Goldberg MF. Surgical management of traumatic hyphema. Ophthalmic Surg. 1983;14(2):137-141.
Crouch ER Jr, Frenkel M. Aminocaproic acid in the treatment of traumatic hyphema. Am J Ophthalmol. 1976;81(3):355-360. doi:10.1016/0002-9394(76)90254-3.
Bansal S, Gunasekeran DV, Ang B, Lee J, Khandelwal R, Sullivan P, et al. Controversies in the pathophysiology and management of hyphema. Survey of ophthalmology. 2016;61(3):297-308. doi:10.1016/j.survophthal.2015.11.005. PMID:26632664.
Malvankar-Mehta MS, Fu A, Subramanian Y, Hutnik CML. Impact of ophthalmic viscosurgical devices in cataract surgery. J Ophthalmol. 2020;2020:7801093. doi:10.1155/2020/7801093. PMID: 33133677; PMCID: PMC7593745.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.