Dacryocystitis is an inflammatory disease caused by pathogenic microorganisms infecting the lacrimal sac due to impaired tear drainage. It is broadly classified into acute dacryocystitis and chronic dacryocystitis.
Acute dacryocystitis is a condition in which acute purulent inflammation spreads from the lacrimal sac to the surrounding tissues. It presents with severe pain, swelling, and redness, and may progress to orbital cellulitis (deep infection of the orbit). Chronic dacryocystitis is a condition in which stenosis or obstruction of the lacrimal sac and nasolacrimal duct leads to accumulation of waste products and mucus, with abnormal bacterial growth. Chronic tearing and discharge are the main symptoms.
Neonatal dacryocystitis is a condition in which secondary infection occurs in congenital nasolacrimal duct obstruction (CNLDO). Dacryolithiasis is a condition in which bacterial stones form in the lacrimal passages, causing recurrent canaliculitis and dacryocystitis, with Actinomyces being the most common causative organism.
The symptomatic incidence of acquired nasolacrimal duct obstruction is 30.47 per 100,000 person-years, with women (43.06 per 100,000 person-years) accounting for approximately 2.4 times that of men (18.01 per 100,000 person-years)10).
Type
Pathophysiology
Predisposition
Main Symptoms
Acute dacryocystitis
Acute purulent inflammation from lacrimal sac to surrounding tissues
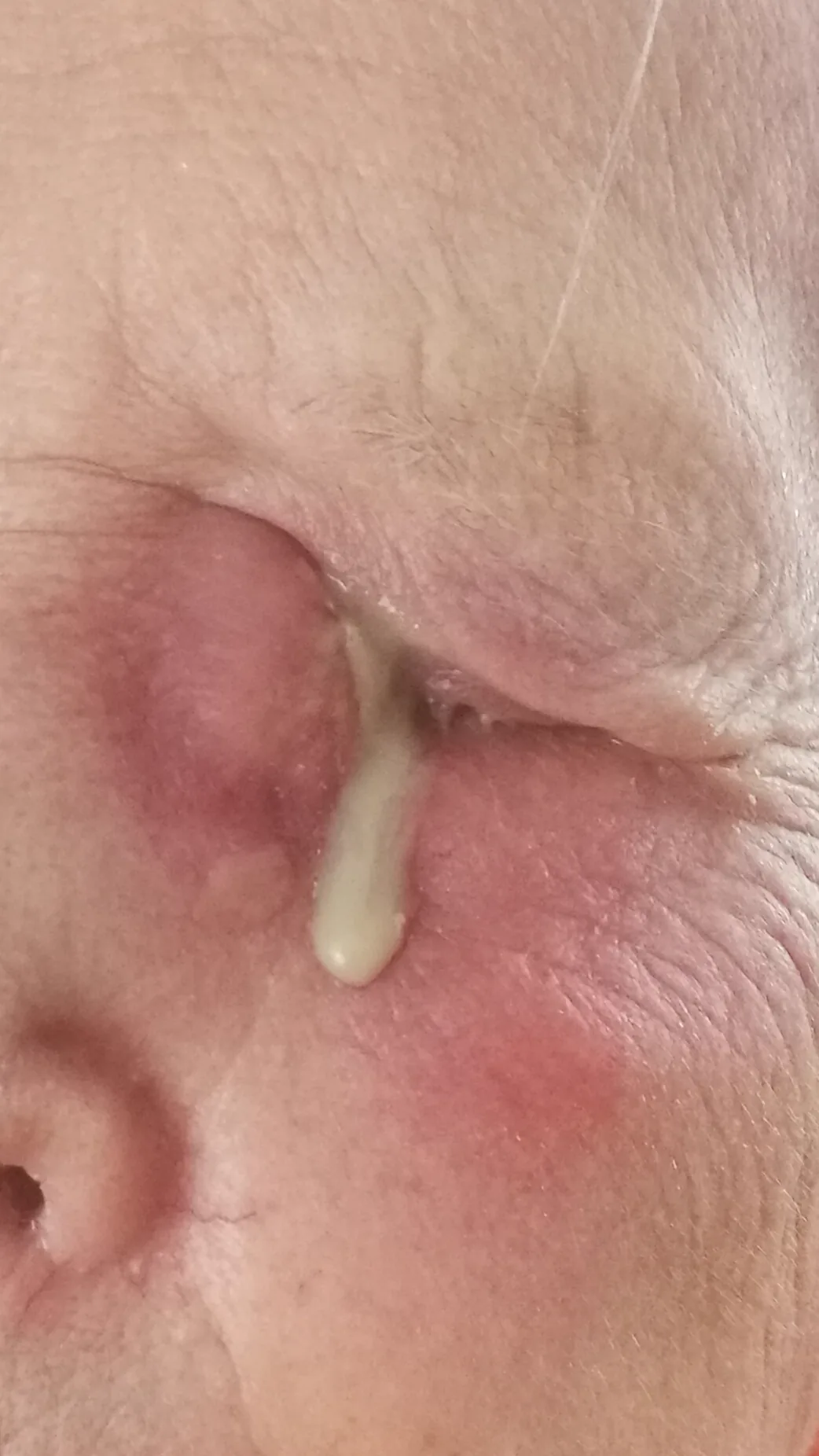
Left acute dacryocystitis in an 80-year-old woman: marked redness, swelling, and skin tightness slightly below the inner canthus (lacrimal sac area), with visible discharge. Corresponds to the visual findings (redness, swelling, tenderness below the inner canthus) of acute dacryocystitis discussed in the section “Main symptoms and clinical findings.”
Symptoms of acute dacryocystitis
Epiphora and discharge: present from early onset
Marked redness, swelling, and pain in the lacrimal sac area: the area slightly below the inner canthus swells and is extremely tender to touch
Progression to orbital cellulitis: if the infection spreads deeply, it can cause proptosis, restricted eye movement, and vision loss
Symptoms of Chronic Dacryocystitis
Epiphora and discharge: Long-lasting persistent symptoms
Mild swelling around the lacrimal sac: Persistent swelling, though less prominent than in acute cases
Acute dacryocystitis often presents with sudden swelling and severe pain below the inner canthus (medial canthus). High fever and general malaise may accompany.
Chronic dacryocystitis primarily presents with epiphora (excessive tearing) and discharge (eye mucus). Patients often visit complaining of “pus-like discharge when pressing the eye” or “persistent redness of the eye that does not resolve.”
Neonatal dacryocystitis presents with swelling of the lacrimal sac area, mucopurulent discharge, and epiphora. Pus reflux is observed upon lacrimal sac irrigation or compression. Reports indicate that common causative organisms include Staphylococcus aureus and Haemophilus influenzae.
Clinical Findings (Findings Confirmed by Physician Examination)
Acute dacryocystitis: Marked redness, swelling, and tenderness below the inner canthus. The skin feels tense. Severe cases may progress to orbital cellulitis, presenting with proptosis and restricted eye movement.
Chronic dacryocystitis: Mild swelling is palpable over the lacrimal sac. Pus reflux from the punctum is confirmed upon lacrimal sac compression or lacrimal irrigation test. The discharged pus is sent for smear microscopy and bacterial culture to identify the causative organism and perform antibiotic sensitivity testing.
Dacryolithiasis: Recurrent dacryocystitis and canaliculitis. Fungal stones are identified microscopically as Gram-positive branching filamentous organisms.
QWhat symptoms lead to the detection of dacryocystitis?
A
Acute dacryocystitis is often noticed due to severe pain, swelling, and redness below the inner canthus. Chronic dacryocystitis is characterized by persistent epiphora and discharge, with pus reflux from the punctum upon pressing the inner canthus. In neonates, swelling near the inner canthus and mucopurulent discharge are the main complaints.
Dacryocystitis often occurs secondary to nasolacrimal duct obstruction in older adults. The nasolacrimal duct in women tends to be anatomically narrower, making it more common in women. The symptomatic incidence of acquired nasolacrimal duct obstruction is 30.47 per 100,000 person-years, with women (43.06 per 100,000 person-years) being approximately 2.4 times more affected than men (18.01 per 100,000 person-years)10). The incidence increases with age, peaking at 70–79 years10). There is no significant difference between races (white vs. non-white)10).
Neonatal dacryocystitis is reported to develop from congenital nasolacrimal duct obstruction (CNLDO) in about 2–4% of cases. The spontaneous resolution rate of CNLDO itself is high at 96% by 12 months of age3). The rate of acute dacryocystitis complicating congenital dacryocystocele (CDC) is reported to be as high as 15.2–75%6).
Treatment outcomes with probing tend to decrease with age: 80–90% at 1 year, 73–84% at 2 years, 65–75% at 3 years, and 63% at 4–5 years5).
Dacryoliths are reported to be present in 7.5% of nasolacrimal duct obstruction cases2) and are a risk factor for acute dacryocystitis.
Dacryocyst compression (Crigler method): Compress the lacrimal sac area below the inner canthus and check for purulent reflux from the punctum. If reflux is observed, dacryocystitis is almost confirmed.
Acute phase inspection: Check for redness, swelling, warmth, and tenderness over the lacrimal sac area. If proptosis or ocular motility disturbance is present, suspect progression to orbital cellulitis.
Lacrimal Irrigation and Examination
Lacrimal irrigation (lacrimal duct patency test): Inject normal saline through the punctum; if pus refluxes, dacryocystitis is confirmed. Also useful for identifying the site of obstruction.
Bacterial culture and smear microscopy: Use discharged pus as a specimen for causative organism identification and antibiotic sensitivity testing.
Lacrimal endoscopy: Allows direct visualization of the lacrimal duct lumen for detailed assessment of obstruction site and mucosal characteristics2).
Imaging Studies
CT scan: Evaluate the orbit and paranasal sinuses to check for extension to orbital cellulitis.
Dacryocystography: Contrast medium is injected through the punctum to identify the site of obstruction.
In acute dacryocystitis, gram-positive bacteria are most common, with Staphylococcus aureus and Streptococcus pneumoniae being representative causative organisms3). In chronic dacryocystitis, in addition to gram-positive bacteria such as Staphylococcus epidermidis and Corynebacterium spp., gram-negative bacteria such as Pseudomonas aeruginosa are also detected4). While aerobic bacteria predominate in acute dacryocystitis, the proportion of anaerobic bacteria increases in chronic dacryocystitis3,4).
Actinomycetes are the most common causative organisms of dacryolithiasis, with anaerobic Actinomyces being the representative species. Diagnosis can be made by identifying Gram-positive, branched filamentous organisms on Gram stain.
Orbital cellulitis: Spread from acute dacryocystitis. Differentiate with CT/MRI
Lacrimal sac tumor: Malignant lymphoma, adenocarcinoma. Tumors are found in 1.4% of DCR surgeries, of which 69% are malignant2). Biopsy is necessary if the mass grows rapidly.
Dermoid cyst: In children, it should be differentiated as a mass near the inner canthus.
Differentiation from tumors—must not be missed
Even with symptoms resembling chronic dacryocystitis, it is important to rule out lacrimal sac tumors. Especially if the mass rapidly enlarges or does not respond to antibiotic therapy, biopsy should be performed during DCR or via diagnostic puncture.
Systemic and topical antibiotics are administered to prevent spread of inflammation. If pain in the lacrimal sac area is severe, puncture and drainage are performed. After inflammation subsides, definitive surgery (DCR) is planned.
Antibiotic therapy:
Topical antibiotics: Levofloxacin ophthalmic solution (1.5%) 4 times daily, or Tosufloxacin ophthalmic solution (0.3%) 4 times daily
Oral antibiotics: Cefdinir 300 mg/day divided into 3 doses, or Amoxicillin/clavulanate combination tablet 1 tablet 3 times daily (7–14 days)
Severe cases (when orbital cellulitis spreads): Ceftriaxone 1–2 g/day intravenous drip
After inflammation subsides, dacryocystorhinostomy (DCR) is planned as a definitive treatment for dacryocystitis. Since drainage alone leads to recurrence, reconstruction of the lacrimal passage is necessary.
Chronic dacryocystitis is difficult to cure with antibiotics alone. The definitive treatment is lacrimal passage reconstruction, requiring lacrimal tube intubation or dacryocystorhinostomy (DCR). The reocclusion rate of lacrimal tube intubation (blind tube placement) for chronic dacryocystitis is high at 45–80%.
DCR achieves a success rate of 90–99% 2). The success rate of lacrimal tube intubation under dacryoendoscopy (DEP/SEP method) is 70–87% at 1 year after tube removal 2). The survival rate at 3,000 days after lacrimal tube removal is 64%, indicating a long-term risk of recurrence 2). Factors associated with recurrence include history of dacryocystitis, long disease duration, long obstruction distance, and male sex 2).
Both external DCR and endonasal DCR show high success rates 4,5). External DCR requires a skin incision but allows direct visualization, and has been reported to have a slightly higher success rate 5). Endonasal DCR (transnasal endoscopic DCR) has the advantage of no skin incision and better cosmetic outcomes 4).
QCan chronic dacryocystitis be cured with medication alone?
A
It is difficult to cure with antibiotics alone. For a radical cure, dacryocystorhinostomy (DCR) is required, with a high success rate of 90–99%. Lacrimal tube alone (blind tube intubation) has a high reocclusion rate of 45–80% and is currently not recommended. Endoscopic lacrimal tube intubation is minimally invasive, but the success rate after one year is 70–87%, not as high as DCR.
QWhat is the difference between external and endoscopic DCR (dacryocystorhinostomy)?
A
External DCR is a classic standard procedure with a skin incision and direct visualization, with a success rate of 90–99%. Endoscopic DCR is performed via nasal endoscopy without skin incision, offering cosmetic benefits, but some reports indicate a slightly lower success rate 8,9). In recent years, there have been increasing reports that both techniques show comparable outcomes depending on the surgeon’s proficiency.
Antibiotic eye drops and lacrimal sac massage are performed. If inflammation or surrounding swelling is severe, systemic antibiotics may also be administered. If no improvement is achieved, probing of the lacrimal duct is performed to open the obstruction of the nasolacrimal duct and drain the pus.
Prescription example:
Tosufloxacin ophthalmic solution (0.3%) 4 times daily
Since the spontaneous resolution rate of CNLDO itself is as high as 96% by 12 months of age 3), observation with antibiotic eye drops and lacrimal sac massage is recommended if there is no acute dacryocystitis 1). Antibiotic eye drops reduce eye discharge and mucopurulent secretions, but there is no evidence that they increase the cure rate, and long-term use carries a risk of resistant bacteria, so they should be used only when necessary 1).
The success rate of probing decreases with age: 80–90% at 1 year, 73–84% at 2 years, 65–75% at 3 years, and 63% at 4–5 years 5). The cure rate of endoscopic probing is high at 92.3–100% 1). For unilateral CNLDO at 6–9 months of age, immediate outpatient probing is weakly recommended (evidence level C) 1).
Congenital dacryocystocele (CDC) complicated by acute dacryocystitis is an indication for early surgical treatment 6).
Since congenital nasolacrimal duct obstruction resolves spontaneously in 96% of cases by 12 months of age3), the basic management is observation with antibiotic eye drops and lacrimal sac massage unless acute dacryocystitis is present1). If there is no improvement, probing is performed. When acute dacryocystitis complicates congenital dacryocystocele, early surgical intervention is indicated6).
The basic treatment is complete removal of the dacryolith from the lacrimal passage. Because it is accompanied by inflammatory pain, adequate local anesthesia (intracanalicular anesthesia and infratrochlear nerve block) should be performed.
Canalicular dacryolith: First, compress the canaliculus to express the stone through the punctum. If a sharp spoon is used, gently curette the inner wall to minimize damage to the canalicular epithelium.
Lacrimal sac dacryolith: Remove using a lacrimal endoscope. Confirmation with a lacrimal endoscope is useful for complete removal2).
Combination with antibiotics: Administer sensitive antibiotics concomitantly.
Lacrimal sac stones are found in 7.5% of nasolacrimal duct obstruction cases; 21 of 23 cases could be removed via the nasolacrimal duct, but 2 cases required DCR due to large size2). Often, a single procedure is insufficient, and multiple procedures may be necessary.
5.5 Chronic dacryocystitis and risk management before intraocular surgery
Chronic dacryocystitis is a risk factor for postoperative endophthalmitis after intraocular surgeries such as cataract surgery. Before intraocular surgery, lacrimal passage evaluation should be performed; if dacryocystitis is confirmed, it is important to normalize the lacrimal passage with DCR or other procedures prior to surgery.
QCan cataract surgery be performed if dacryocystitis is present?
A
Because chronic dacryocystitis is a risk for postoperative endophthalmitis, lacrimal passage evaluation should be performed before intraocular surgeries such as cataract surgery. If dacryocystitis is confirmed, treatment (e.g., DCR) should be performed first, followed by intraocular surgery. Once normalization of the lacrimal passage is confirmed, surgery can be performed with standard risk management.
The tear drainage pathway runs sequentially: superior and inferior lacrimal puncta → lacrimal canaliculi (vertical part 2 mm + horizontal part 8 mm) → common canaliculus → lacrimal sac (approximately 12 mm long) → nasolacrimal duct (approximately 12 mm long) → inferior nasal meatus. The lacrimal sac is located in the bony lacrimal fossa (between the anterior and posterior lacrimal crests). At the lower end of the nasolacrimal duct, there is a mucosal valve called the valve of Hasner. Incomplete opening of this valve is the main cause of congenital nasolacrimal duct obstruction (CNLDO)1).
Acute dacryocystitis:
Nasolacrimal duct obstruction → bacterial proliferation in the lacrimal sac → acute suppurative inflammation → spread to surrounding tissues. If it progresses to orbital cellulitis, it can affect vision and eye movement.
Chronic dacryocystitis:
Stenosis of the lacrimal drainage system → accumulation of waste products and secretions → proliferation of anaerobic bacteria → chronic inflammation. Persistent chronic inflammation leads to thickening and fibrosis of the nasolacrimal duct mucosa, creating a vicious cycle that worsens the obstruction.
Dacryolithiasis:
Actinomyces israelii forms colonies within the lumen, creating stones. These stones obstruct the lumen and cause dacryocystitis and canaliculitis. Gram-positive branching filamentous bacteria are characteristic findings and can be identified by Gram staining.
Neonatal dacryocystitis:
Incomplete opening of the valve of Hasner (congenital nasolacrimal duct obstruction) leads to accumulation of secretions in the lacrimal sac, which then becomes secondarily infected by Staphylococcus aureus, Haemophilus influenzae, etc. Cases with early formation of a lacrimal sac mucocele (congenital dacryocystocele) have a particularly high rate of acute dacryocystitis1,6).
Acute dacryocystitis:
Appropriate antibiotic therapy and, if necessary, puncture and drainage can achieve resolution of inflammation, but definitive treatment requires dacryocystorhinostomy (DCR). Since nasolacrimal duct obstruction persists after inflammation subsides, acute dacryocystitis may recur if left untreated. If inflammation is not controlled, it can progress to perisac abscess and formation of a cutaneous fistula.
Chronic dacryocystitis:
The success rate of DCR is 90–99%2), and high cure rates can be expected when surgery is performed at an appropriate time. Endoscopic transcanalicular tube placement is minimally invasive, but the survival rate (patency rate) at 3,000 days after tube removal is 64%2), so it is important to fully explain the long-term risk of recurrence. Risk factors for recurrence include a history of dacryocystitis, long disease duration, long obstruction length, and male sex2). Chronic dacryocystitis is a risk factor for postoperative endophthalmitis after intraocular surgery, so lacrimal drainage evaluation before cataract surgery is important.
Neonatal dacryocystitis:
The spontaneous resolution rate of CNLDO is as high as 96% by 12 months of age3). The cure rate with probing is higher when performed at a younger age, and it is desirable to perform it before 1 year of age5). Endoscopic transcanalicular probing has been reported to achieve a high cure rate of 92.3–100%1).
Dacryolithiasis:
Prognosis is good if the dacryolith is completely removed. However, it is often not possible to remove it in a single procedure, and multiple procedures may be required.
Mills DM, Bodman MG, Meyer DR, Morton AD 3rd; ASOPRS Dacryocystitis Study Group. The microbiologic spectrum of dacryocystitis: a national study of acute versus chronic infection. Ophthalmic Plast Reconstr Surg. 2007;23(4):302-306.
Bharathi MJ, Ramakrishnan R, Maneksha V, Shivakumar C, Nithya V, Mittal S. Comparative bacteriology of acute and chronic dacryocystitis. Eye (Lond). 2008;22(7):953-960.
Kashkouli MB, Kassaee A, Tabatabaee Z. Initial nasolacrimal duct probing in children under age 5: cure rate and factors affecting success. J AAPOS. 2002;6(6):360-363.
Lueder GT. The association of neonatal dacryocystoceles and infantile dacryocystitis with nasolacrimal duct cysts (an American Ophthalmological Society thesis). Trans Am Ophthalmol Soc. 2012;110:74-93.
Pediatric Eye Disease Investigator Group. Resolution of congenital nasolacrimal duct obstruction with nonsurgical management. Arch Ophthalmol. 2012;130(6):730-734.
Woog JJ. The incidence of symptomatic acquired lacrimal outflow obstruction among residents of Olmsted County, Minnesota, 1976-2000 (an American Ophthalmological Society thesis). Trans Am Ophthalmol Soc. 2007;105:649-666.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.

{kind=link}