Ocular Ischemic Syndrome (OIS) is a general term for ocular disorders caused by chronic reduction of ocular blood flow 1). It is most commonly caused by carotid artery stenosis due to atherosclerosis. Inflammatory diseases such as Takayasu arteritis and giant cell arteritis can also cause stenosis.
Severe stenosis of the internal carotid artery (ICA) or common carotid artery (CCA) leads to decreased perfusion pressure in the ophthalmic artery, causing ipsilateral ocular damage. The condition in which ocular and neurological symptoms appear due to decreased ophthalmic artery blood flow and blood pressure associated with internal carotid artery occlusion or stenosis is also called “internal carotid artery syndrome” 5). Since OIS carries a risk of cerebral infarction, collaboration with other departments is important.
Lesions are classified into the following two types based on the mode of onset:
Age of onset: mean age approximately 65 years. Onset before age 50 is rare.
Sex difference: male-to-female ratio 2:1, more common in men. This is attributed to the higher incidence of arteriosclerosis and carotid artery disease in men.
Bilaterality: up to 22% of cases develop in both eyes2).
Incidence: estimated at approximately 7.5 cases per 100,000 population per year9). However, misdiagnosis as retinal vein occlusion or diabetic retinopathy may lead to underestimation.
Association with diabetes: Patients with internal carotid artery occlusion often have diabetes.
In symptomatic carotid artery occlusion patients, asymptomatic retinal vascular changes are observed in about 29%, and some progress to symptomatic OIS9).
QIs OIS always unilateral?
A
About 20% develop in both eyes2). This is more likely when stenosis affects both carotid arteries. Severity varies depending on the degree of stenosis, development of collateral circulation, and presence of systemic vascular disease.
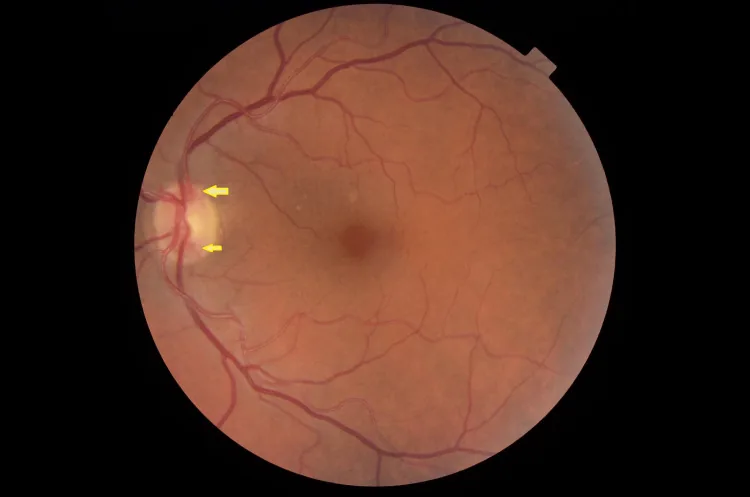
Metry Y, et al. Optic DiscNeovascularization as the Only Sign of Ocular Ischemic Syndrome: A Case Report. Cureus. 2022. Figure 1. PMCID: PMC9636562. License: CC BY.
Arrow indicates optic discneovascularization in the left eye. This corresponds to the disc neovascularization discussed in the section “2. Main symptoms and clinical findings”.
OIS is an ocular manifestation of a systemic disease, and patients may present with systemic symptoms rather than ocular symptoms. The main subjective symptoms are as follows.
Visual loss: Often progresses gradually, but can also occur suddenly. One report indicates that 65% of patients have visual acuity of 20/400 (0.05) or worse at the initial visit4).
Amaurosis fugax: Observed in about 10% of patients9). A dark shadow spreads across the entire visual field and lasts for seconds to minutes. The main cause is transient embolism of the central retinal artery or its branches.
Ocular pain: Present in about 40% of patients9). It is a dull, persistent pain occurring in the upper orbit, upper face, and temporal region. It worsens in the upright position and improves when lying down. It is also called “ocular angina”.
Ocular signs of OIS can be divided into anterior segment, posterior segment, and orbital findings.
Anterior segment findings
Rubeosis iridis: The most characteristic anterior segment finding, occurring in 67% of cases7). It can cause neovascular glaucoma.
Intraocular pressure fluctuation: In half of patients with rubeosis iridis, intraocular pressure rises. In the other half, pressure does not rise due to decreased aqueous humor production by the ciliary body.
Anterior chamber inflammation: Flare and cell increase are observed. Similar to iridocyclitis.
QWhy may intraocular pressure not rise despite the presence of iris rubeosis?
A
In OIS, chronic ischemia reduces aqueous humor production by the ciliary body. Therefore, even if iris rubeosis obstructs the aqueous outflow pathway, intraocular pressure may remain normal or low due to decreased aqueous production. For details, see the “Pathophysiology” section.
The main cause of OIS is stenosis or occlusion of the carotid artery due to arteriosclerosis. The following risk factors are involved.
Arteriosclerosis: The most common cause. It involves lipid deposition, fibrous thickening, atheroma, and thrombus formation in the intima of large and medium arteries.
Diabetes: Diabetes is frequently associated with internal carotid artery occlusion.
Hypertension: A major systemic risk factor that promotes arteriosclerosis.
Hyperlipidemia, smoking, and advanced age: All increase the risk of carotid artery disease.
Inflammatory diseases: Aortitis syndrome (Takayasu arteritis) and giant cell arteritis can cause carotid artery stenosis. Takayasu arteritis causes inflammatory stenosis of the aortic arch branches and differs from typical arteriosclerotic OIS in that it is more common in relatively young individuals (women under 40). Giant cell arteritis is more common in older adults over 50 and may be accompanied by jaw claudication, headache, and tenderness of the temporal artery.
If collateral circulation is healthy, OIS may not develop even if the ICA is completely occluded. Conversely, if collateral circulation is insufficient, OIS can develop even with approximately 50% ICA stenosis 8,9).
Delayed choroidal filling: The most specific angiographic finding. Observed in 60% of OIS eyes9). Normally completed within 5 seconds after contrast appearance, choroidal filling is markedly delayed. This is also reflected as “delayed arm-to-retina circulation time,” prolonging the time for contrast to reach the fundus from the arm.
Prolonged retinal arteriovenous transit time: The most sensitive angiographic finding. It is observed in up to 95% of eyes9), and some cases show a delay of 1 minute or more.
Retinal vessel staining: observed in 85% of cases9). It results from damage to vascular endothelial cells due to breakdown of the inner blood-retinal barrier. Arterial staining is particularly prominent in OIS and is useful for differentiating from CRVO.
It allows more detailed evaluation of choroidal vascular abnormalities. In OIS, prolonged arm-to-choroid circulation time and intrachoroidal circulation time are observed. Filling defects appear due to occlusion of the choriocapillaris.
Electroretinography (ERG)/VEP: OIS may show electrophysiological abnormalities depending on the degree of ischemia, but the mainstay of diagnosis is fluorescein angiography and carotid artery imaging9).
VEP: It is sometimes used as an adjunctive test, and some reports show improvement after revascularization14).
The following tests are used to evaluate carotid artery stenosis.
Test
Features
Sensitivity/Specificity
Carotid duplex ultrasound
First choice. Noninvasive.
Detection of occlusion: sensitivity 96%, specificity 100%11)
MRA
Secondary detailed examination
70–99% stenosis: sensitivity 95%, specificity 90%
CTA
Allows simultaneous evaluation of cerebrovascular disorders
Excellent for plaque characterization
The relationship between peak systolic velocity (PSV) on carotid duplex ultrasound and ICA stenosis rate varies depending on facility standards and measurement conditions, but typical reference values are as follows11,12).
PSV 125–225 cm/sec → 50–70% ICA stenosis
PSV 225–350 cm/sec → 70–90% ICA stenosis
PSV > 350 cm/sec → >90% ICA stenosis
On color Doppler imaging, reversed flow pattern in the ophthalmic artery is a specific indicator of ipsilateral high-grade ICA stenosis or occlusion.
Often accompanied by findings other than hemorrhage, such as cotton-wool spots and hard exudates. FA shows no arterial staining, mainly venous leakage.
In differentiating from CRVO, FA shows strong leakage from retinal veins in CRVO, whereas in OIS, arterial staining is more prominent than venous staining. CRVO may have collateral vessels (loop-like vessels) on the optic disc, which are not seen in OIS.
QHow to differentiate OIS from diabetic retinopathy?
A
In OIS, FA shows delayed choroidal filling and prominent retinal artery staining, with mild proliferative changes. In diabetic retinopathy, leakage from veins is predominant and choroidal filling is normal. Since OIS and diabetic retinopathy can coexist, consider both diseases if neovascularization is present despite mild fundus findings.
Surgical treatment for carotid artery stenosis is the fundamental therapy to restore ocular blood flow. For symptomatic high-grade ICA stenosis, the indications for carotid endarterectomy (CEA) or stenting should be discussed with neurosurgeons and vascular surgeons from the perspective of stroke prevention and improvement of ocular blood flow. Improvements in ocular hemodynamics and electrophysiological findings have been reported after revascularization 13,14).
For patients at high surgical risk, superficial temporal artery to middle cerebral artery (STA-MCA) bypass may be considered as an invasive treatment option. This is a bypass procedure aimed at improving cerebral blood flow in cases where CEA or carotid artery stenting is difficult, and the indication is determined in collaboration with neurosurgeons.
The stepwise treatment decision process is shown below.
Evaluation of carotid artery stenosis: Assess the degree of stenosis and plaque characteristics using carotid ultrasound, MRA, and CTA.
Collaboration with internal medicine and neurosurgery: Determine the indication for CEA or carotid artery stenting. Also consider concurrent medical treatments such as anticoagulation therapy and vasodilator therapy.
Cases with rubeosis iridis: Perform panretinal photocoagulation (PRP) to suppress VEGF production from the ischemic retina.
Cases with neovascular glaucoma: Start intraocular pressure-lowering medications. If intraocular pressure cannot be controlled, consider filtration surgery or cyclophotocoagulation depending on residual visual function.
Adjunctive treatment: Intravitreal injection of VEGF inhibitors has been reported at the case report level to temporarily regress neovascularization (not covered by insurance)15).
Intravitreal anti-VEGF injection: Intravitreal administration of VEGF inhibitory antibodies has been reported at the case report level to temporarily regress neovascularization (not covered by insurance)15). It is also useful as an adjunct to PRP to improve visibility when vitreous hemorrhage is present. Stable regression without fundamental improvement in ocular blood flow is difficult to expect.
Glaucoma surgery: If intraocular pressure does not decrease with PRP, consider filtration surgery or cyclophotocoagulation depending on residual visual function.
Antiplatelet therapy: Initiate in collaboration with internal medicine for prevention of cerebral infarction.
Anticoagulation therapy/Vasodilator therapy: Used as adjunctive medical treatment. Stellate ganglion block may also be considered to improve blood flow.
Management of systemic vascular risk factors: Control hypertension, diabetes, and hyperlipidemia, and provide smoking cessation guidance.
Search for cardioembolism: Evaluation for atrial fibrillation via echocardiography and electrocardiography is necessary.
QCan anti-VEGF drugs be a fundamental treatment for OIS?
A
Intravitreal injection of anti-VEGF drugs can temporarily regress neovascularization associated with OIS, but it is not covered by insurance and is not a fundamental treatment. It is used as an adjunct to panretinal photocoagulation or to improve visibility during vitreous hemorrhage. The fundamental treatment for OIS is carotid revascularization (e.g., CEA), and stable regression of neovascularization without improvement in ocular blood flow is unlikely.
The development of OIS involves insufficiency of collateral circulation between the ICA and ECA systems or between the left and right ICAs. The development of collateral circulation varies greatly among individuals and is one of the most important factors determining the onset and severity of the disease.
In OIS eyes, blood flow in the retrobulbar vessels decreases, and reversal of blood flow in the ophthalmic artery occurs 10). The ophthalmic artery functions as a “steal artery,” and a state of low perfusion persists. Diastolic blood pressure in the ophthalmic artery decreases and improves/normalizes after carotid artery surgery.
Severe stenosis of the internal carotid artery or common carotid artery → decreased ophthalmic artery perfusion pressure → chronic ischemia of the ipsilateral retina, iris, and choroid: this series of hemodynamic changes forms the basis of OIS.
Choroidal ischemia: Occlusion of the choriocapillaris occurs, reducing oxygen and nutrient supply to the outer retina (photoreceptors). This is reflected as a decrease in the a-wave amplitude on ERG.
Inner retinal ischemia: Reduced perfusion pressure in the central retinal artery leads to ischemia of the inner retina. This is detected as a decrease in the b-wave amplitude on ERG.
Neovascularization: Increased VEGF production due to chronic ischemia causes rubeosis iridis, optic discneovascularization, and retinal neovascularization. The cascade of chronic ischemia → VEGF overexpression → rubeosis iridis → angle closure → neovascular glaucoma determines the visual prognosis in OIS.
Breakdown of the blood-retinal barrier: Chronic ischemia damages the inner blood-retinal barrier, observed as staining of retinal vessels and increased flare.
Ciliary body ischemia and reduced aqueous humor production
Chronic ciliary body ischemia reduces the aqueous humor production function of the ciliary epithelium. Therefore, even if iris rubeosis causes obstruction of the aqueous outflow pathway, the decrease in aqueous humor production may offset this, and intraocular pressure may remain normal to low. In OIS eyes before the onset of iris rubeosis, intraocular pressure is often normal or tends to be low.
This mechanism produces a characteristic clinical picture of OIS, where intraocular pressure does not rise despite the presence of iris rubeosis. Furthermore, if ciliary body function recovers after revascularization by CEA, aqueous humor production may increase and intraocular pressure may rise.
In atherosclerosis of the internal carotid artery, lipid deposition, fibrous thickening, and atheroma formation occur in the intima. This narrows the vascular lumen and reduces downstream perfusion pressure. Emboli released from the stenotic site may occlude retinal artery branches (causing amaurosis fugax).
The visual prognosis of OIS is largely determined by the presence or absence of iris rubeosis.
Cases with iris rubeosis: Visual outcomes tend to be poor, and progression to neovascular glaucoma is a major cause of visual deterioration3,9,16).
Cases without iris rubeosis: Relatively good visual prognosis can be expected.
Life prognosis: Because OIS carries a risk of cerebral infarction, long-term management of atherosclerotic risk factors (hypertension, diabetes, dyslipidemia, smoking) is directly linked to life prognosis.
Factors that influence visual prognosis are as follows.
Presence of rubeosis iridis: The most important prognostic factor. When rubeosis iridis develops, it progresses to neovascular glaucoma, and visual function rapidly deteriorates.
Success of carotid artery revascularization: Successful revascularization via CEA may improve ocular blood flow and halt the progression of vision loss. However, advanced ischemic changes are irreversible.
Visual acuity at initial presentation: Patients with good initial visual acuity (20/400 or better) tend to have a relatively favorable prognosis.
Management of systemic diseases: Poor control of arteriosclerosis, diabetes, and hypertension tends to worsen ocular symptoms.
Collaboration with other departments and long-term management
OIS patients require collaboration not only with ophthalmology but also with the following departments.
Neurosurgery/Vascular Surgery: Evaluation and performance of surgical treatment for carotid artery stenosis (CEA/stenting).
Cardiology/Neurology: Prevention and management of cerebral infarction and cardiovascular events. Management of antiplatelet and anticoagulant medications.
Internal Medicine/Diabetology: Control of vascular risk factors (hypertension, diabetes, dyslipidemia).
OCT angiography (OCTA) is a technique that can visualize retinal and choroidal vascular structures without the use of contrast agents, and its application in evaluating retinal capillary non-perfusion areas in OIS is expected. It is being positioned as a complementary test to fluorescein angiography, but large-scale studies on the usefulness of OCTA in OIS are currently limited.
Carotid artery stenting is being investigated as a less invasive revascularization method alternative to carotid endarterectomy. It is attracting attention as an option for patients at high surgical risk, but evidence on long-term visual outcomes specific to OIS has not been sufficiently accumulated.
Sivalingam A, Brown GC, Magargal LE. The ocular ischemic syndrome. III. Visual prognosis and the effect of treatment. Int Ophthalmol. 1991;15(1):15-20. doi:10.1007/BF00150974. PMID:2010264.
Brown GC, Magargal LE. The ocular ischemic syndrome. Clinical, fluorescein angiographic and carotid angiographic features. Int Ophthalmol. 1988;11(4):239-51. doi:10.1007/BF00131023. PMID:3182177.
Kearns TP, Hollenhorst RW. Venous-stasis retinopathy of occlusive disease of the carotid artery. Proc Staff Meet Mayo Clin. 1963;38:304-312.
Malhotra R, Gregory-Evans K. Management of ocular ischaemic syndrome. Br J Ophthalmol. 2000;84(12):1428-31. doi:10.1136/bjo.84.12.1428. PMID:11090489. PMCID:PMC1723350.
Duker JS, Belmont JB. Ocular ischemic syndrome secondary to carotid artery dissection. Am J Ophthalmol. 1988;106(6):750-2. doi:10.1016/0002-9394(88)90721-0. PMID:3195661.
Terelak-Borys B, Skonieczna K, Grabska-Liberek I. Ocular ischemic syndrome - a systematic review. Med Sci Monit. 2012;18(8):RA138-144. PMCID: PMC3560693. PMID: 22847215
Costa VP, Kuzniec S, Molnar LJ, et al. Clinical findings and hemodynamic changes associated with severe occlusive carotid artery disease. Ophthalmology. 1997;104(12):1994-2002. PMID: 9400757
Grant EG, Benson CB, Moneta GL, et al. Carotid artery stenosis: gray-scale and Doppler US diagnosis—Society of Radiologists in Ultrasound Consensus Conference. Radiology. 2003;229(2):340-346. PMID: 14500855
Alexandrov AV, Bladin CF, Maggisano R, Norris JW. Measuring carotid stenosis. Time for a reappraisal. Stroke. 1993;24(9):1292-6. doi:10.1161/01.str.24.9.1292. PMID:8362420.
Kerty E, Eide N, Hørven I. Ocular hemodynamic changes in patients with high-grade carotid occlusive disease and development of chronic ocular ischaemia. II. Clinical findings. Acta Ophthalmol Scand. 1995;73(1):72-6. doi:10.1111/j.1600-0420.1995.tb00017.x. PMID:7543004.
Kearns TP. Ophthalmology and the carotid artery. Am J Ophthalmol. 1979;88(4):714-22. doi:10.1016/0002-9394(79)90671-8. PMID:507143.
Lee SJ, Lee JJ, Kim SY, Kim SD. Intravitreal bevacizumab (Avastin) treatment of neovascular glaucoma in ocular ischemic syndrome. Korean J Ophthalmol. 2009;23(2):132-4. doi:10.3341/kjo.2009.23.2.132. PMID:19568367. PMCID:PMC2694293.
Chen CS, Miller NR. Ocular ischemic syndrome: review of clinical presentation, etiology, investigation, and management. Compr Ophthalmol Update. 2007;8(1):17-28.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.