Pregnancy causes widespread physiological effects throughout the body, including an increase in circulating blood volume (approximately 40–50%), dramatic hormonal changes (elevated estrogen, progesterone, and cortisol), and alterations in immune status. These changes directly and indirectly affect the eyes, leading to various ophthalmic events ranging from physiological changes to pathological changes that can threaten life or vision 1).
Ophthalmic changes associated with pregnancy can be broadly divided into reversible physiological changes and pathological changes requiring active intervention.
The main ophthalmic changes related to pregnancy are summarized below.
Common in the third trimester; elevated cortisol is involved12)
The decrease in intraocular pressure during pregnancy is a favorable change for glaucoma management, but it also provides an opportunity to review the safety of current eye drops. Refractive surgery (LASIK, ICL, etc.) is contraindicated during pregnancy due to refractive instability and should be considered only after at least 6 months postpartum when refraction has stabilized3).
QCan vision change during pregnancy?
A
Yes. Hormonal changes can alter corneal shape, lens thickness, and intraocular pressure, causing temporary refractive changes (a tendency toward myopia). Corneal edema or curvature changes may also cause discomfort with contact lenses. These changes often resolve after delivery, but if a change in eyeglass prescription is made due to refractive changes during pregnancy, re-evaluation after delivery is necessary.
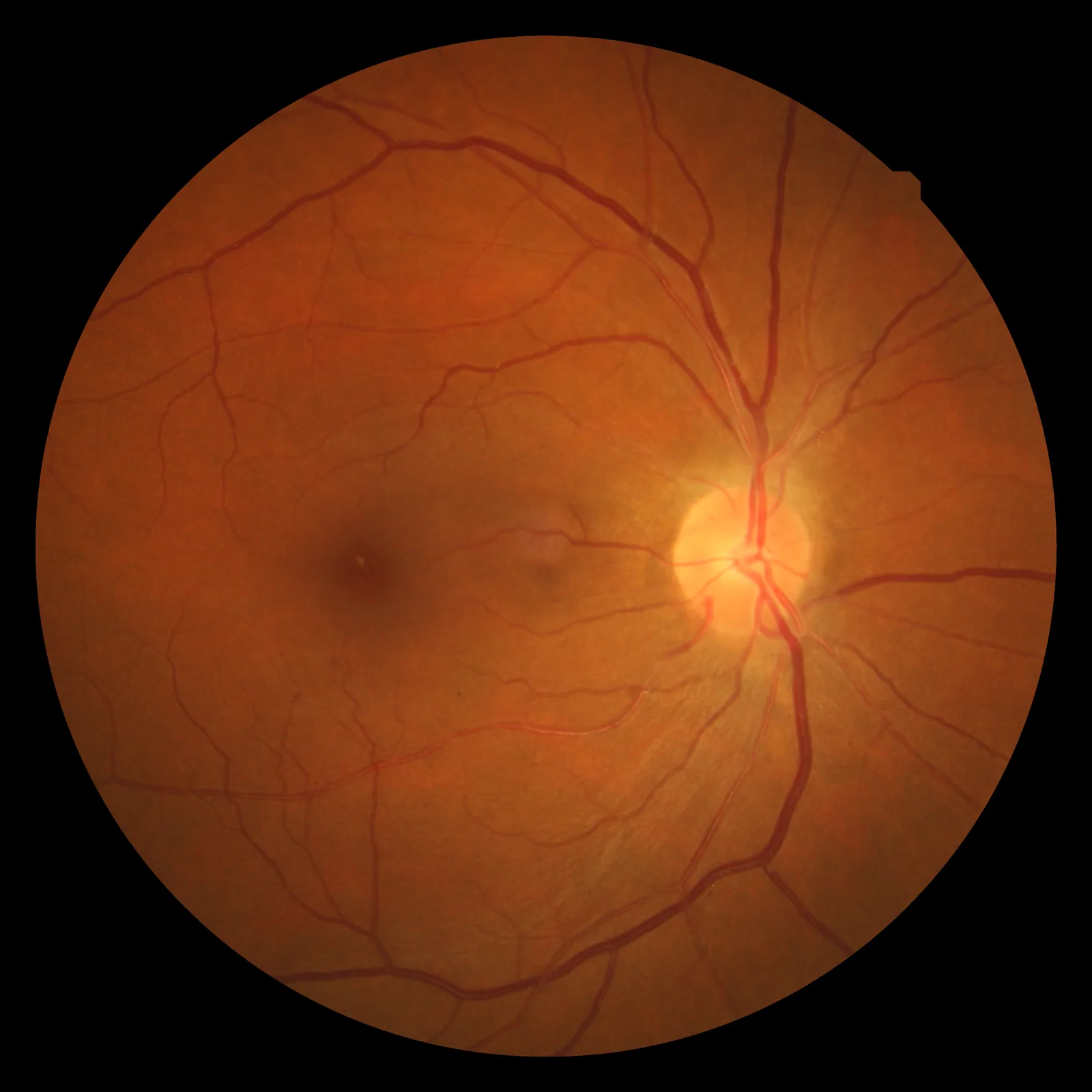
Wood F. Hypertensive retinopathy fundus photograph. Wikimedia Commons. 2009. Figure 1. Source ID: commons.wikimedia.org/wiki/File:Hypertensiveretinopathy.jpg. License: CC BY 3.0.
Fundus photograph of hypertensive retinopathy showing narrowing of retinal arteries, silver-wire arterioles, flame-shaped hemorrhages, and cotton-wool spots (soft exudates). This corresponds to retinal changes due to preeclampsia discussed in section “2. Main Symptoms and Clinical Findings.”
Ocular symptoms during pregnancy vary depending on the underlying disease.
Related to preeclampsia:
Blurred vision (haziness)
Scintillations (flashing lights) and photopsia
Scotomas and visual field defects
Transient visual disturbances
Accompanying headache and edema (systemic symptoms)
The above visual symptoms are signs of worsening preeclampsia and are risk indicators for eclampsia 6). Prompt consultation with an obstetrician and ophthalmologist is recommended.
Increase in microaneurysms: Worsening of existing lesions or new appearance.
Macular edema: Serous or cystoid edema confirmed on OCT.
Neovascularization: Indicates progression from nonproliferative to proliferative DR.
Vitreous hemorrhage: Can cause sudden vision loss due to progression of proliferative DR.
CSC
Serous retinal detachment: Shallow serous retinal detachment localized to the macula.
OCT findings: Subretinal fluid accumulation is clearly visualized.
Fluorescein angiography: Performed only when necessary. Patterns include diffuse or pinpoint leakage.
Cortical Blindness (PRES)
Visual acuity: Transient complete to severe vision loss (bilateral).
Fundus findings: Often normal or only mildly abnormal.
Imaging: MRI/CT shows vasogenic edema in the occipital lobe (coordinate with neurology/obstetrics).
Course: Usually reversible with appropriate blood pressure control and MgSO₄ administration.
QIs it dangerous to have flickering vision or blurred vision during pregnancy?
A
Flashes of light (photopsia) and blurred vision may be signs of worsening preeclampsia. Especially when accompanied by headache, swelling of the limbs, and elevated blood pressure, there is a risk of progression from preeclampsia to eclampsia (seizures). If these symptoms appear, it is important to immediately consult an obstetrician and also undergo an ophthalmological evaluation.
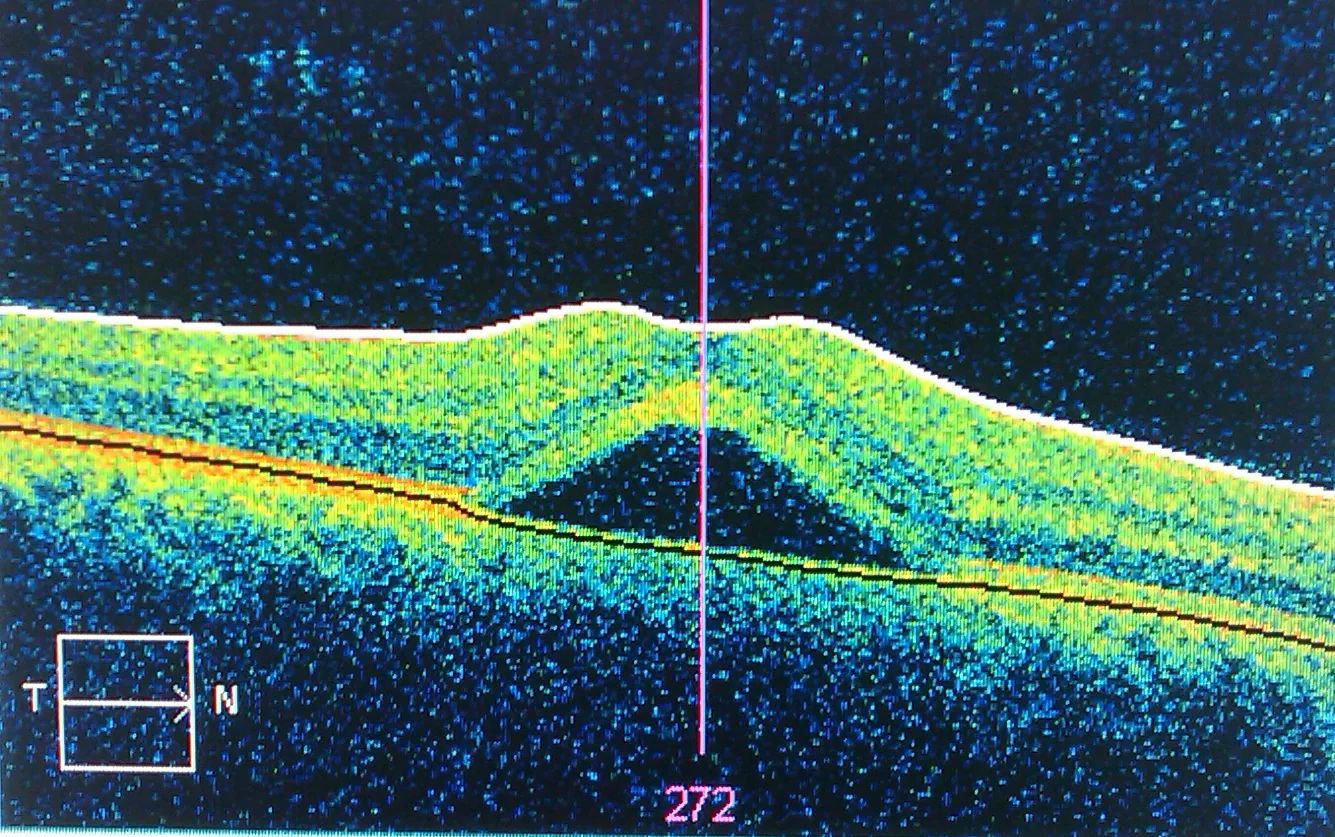
Neches R. Central serous retinopathy OCT scan. Wikimedia Commons. 2010. Figure 1. Source ID: commons.wikimedia.org/wiki/File:Central_serous_retinopathy.jpg. License: CC BY-SA 3.0.
Optical coherence tomography (OCT) shows serous retinal detachment (elevation of the neurosensory retina) and separation from the retinal pigment epithelium (RPE) in the macula. This corresponds to CSC (central serous chorioretinopathy) during pregnancy, discussed in the section “3. Causes and Risk Factors.”
Preeclampsia is a condition characterized by persistent systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg after 20 weeks of gestation 4). The following mechanisms are important in the development of its ocular manifestations.
Systemic vascular endothelial damage → spasm and ischemia of retinal arteries
Overproduction of anti-angiogenic factors (sFlt-1) → decreased activity of VEGF and PlGF (placental growth factor)
Decreased VEGF/PlGF activity → reduced choroidal perfusion → breakdown of the RPE (retinal pigment epithelium) barrier
Breakdown of the RPE barrier → fluid accumulation under the retina → serous retinal detachment
Vasogenic edema of the occipital lobe → PRES → cortical blindness (reversible) 6)
Risk factors for preeclampsia:
Primipara
Multiple pregnancy
Advanced maternal age (≥35 years)
High BMI (25 or higher)
History of hypertension, diabetes, or kidney disease
History of preeclampsia in a previous pregnancy
Worsening of Diabetic Retinopathy During Pregnancy
Pregnancy is an independent risk factor for progression of diabetic retinopathy (DR), and caution is especially needed in diabetic patients with pre-existing DR 7, 8).
The following mechanisms are involved in the worsening:
Increased insulin resistance during pregnancy → amplified blood glucose fluctuations
Elevated endogenous cortisol during pregnancy (especially in the third trimester) is thought to increase choroidal vascular permeability and induce CSC. Pregnancy-associated CSC often resolves spontaneously after delivery, but persistent cases can affect vision 12).
Mechanisms of intraocular pressure reduction and corneal changes
Fundus examination: Evaluation of hypertensive fundus changes according to the Keith-Wagener-Barker classification.
OCT: Detection and quantitative evaluation of serous retinal detachment and retinal edema.
If cortical blindness is suspected: MRI/CT to confirm occipital lobe edema (coordinate with neurology).
QWill the dilating drops used for fundus examination during pregnancy affect the baby?
A
Standard doses of mydriatic agents (tropicamide/phenylephrine eye drops) are considered safe for use during pregnancy when administered appropriately. However, it is recommended to minimize systemic absorption by gently pressing the lacrimal sac (inner corner of the eye) after instillation. For pregnant women with diabetic retinopathy, dilated fundus examination is essential to prevent vision loss, and the benefits far outweigh the risks.
Nonproliferative DR (NPDR): Regular fundus examinations each trimester. Consider photocoagulation if worsening occurs
Progression of proliferative DR (PDR): Panretinal photocoagulation (PRP) can be performed during pregnancy. Laser photocoagulation has established safety for the fetus
Diabetic macular edema (DME): Anti-VEGF agents are contraindicated during pregnancy (teratogenicity reported in animal studies). Reassess after delivery and initiate anti-VEGF therapy if needed9)
Glycemic control: Rapid improvement of HbA1c carries a risk of early worsening. Gradual improvement (decrease of about 0.5–1% per month) is desirable8)
Management of Central Serous Chorioretinopathy (CSC)
For patients using eye drops (e.g., for glaucoma) who become pregnant or are breastfeeding, safety evaluation of the medication is necessary. The safety classification of major glaucoma eye drops is shown below13, 14).
Drug Class
Representative Drug
Assessment During Pregnancy
Assessment During Breastfeeding
Prostaglandin analogs
Latanoprost, bimatoprost
Contraindicated in principle (risk of uterine contractions)
Caution
Beta-blockers
Timolol, carteolol
Caution (risk of fetal bradycardia)
Caution
Alpha-2 agonists
Brimonidine
Caution (risk of central nervous system depression)
Contraindicated during breastfeeding (risk of neonatal respiratory depression)
If continuing beta-blocker eye drops (e.g., timolol), thoroughly perform lacrimal sac compression (press the inner corner of the eye for 1–2 minutes immediately after instillation) to minimize systemic absorption. Brimonidine during breastfeeding carries a risk of central nervous system depression in the newborn and should generally not be used while nursing.
QCan I continue using glaucoma eye drops during pregnancy?
A
Safety varies greatly by medication. Prostaglandin analogs (e.g., latanoprost) may induce uterine contractions and are generally contraindicated during pregnancy. Beta-blockers (e.g., timolol) require caution for fetal bradycardia but may be continued with thorough lacrimal sac compression in some cases. Once pregnancy is confirmed, always consult your ophthalmologist and obstetrician to consider switching to a safe alternative. Neglecting glaucoma control can also lead to progression of visual field loss, so individualized assessment by a specialist is important.
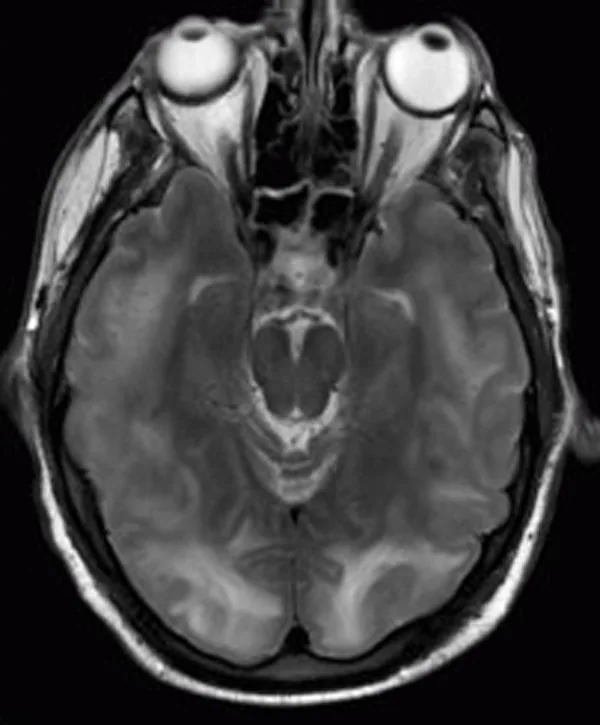
Chawla R, Smith D, Marik PE. Near fatal posterior reversible encephalopathy syndrome complicating chronic liver failure. J Med Case Rep. 2009;3:6623. Figure 2. PMID: 19830117; PMCID: PMC2726521. DOI: 10.1186/1752-1947-3-6623. License: CC BY 3.0.
Brain MRI FLAIR image shows multiple subcortical hyperintense areas in the bilateral occipital lobes, parietal lobes, and pons, indicating vasogenic edema due to posterior reversible encephalopathy syndrome (PRES). This corresponds to cortical blindness (PRES) discussed in section “6. Pathophysiology and Detailed Mechanisms.”
Ocular involvement in preeclampsia arises from a complex mechanism based on systemic endothelial dysfunction5, 6).
Excessive production of the anti-angiogenic factor sFlt-1 (soluble Flt-1) from the placenta increases in the circulation, capturing and inactivating VEGF (vascular endothelial growth factor) and PlGF (placental growth factor). This results in systemic endothelial dysfunction, leading to hypertension, proteinuria, and edema.
Cortical blindness due to PRES (posterior reversible encephalopathy syndrome) is a transient, reversible condition resulting from occipital hyperperfusion and blood-brain barrier disruption, and it resolves with appropriate blood pressure control and anticonvulsant therapy.
Mechanisms of Diabetic Retinopathy Worsening During Pregnancy
Worsening of diabetic retinopathy (DR) during pregnancy involves multiple interacting mechanisms. Increased insulin resistance amplifies blood glucose fluctuations, while increased circulating blood volume (approximately 40–50%) raises retinal blood flow, placing stress on existing microvascular lesions7, 8).
Elevations in growth hormone, prolactin, and IGF-1 promote angiogenesis and stimulate VEGF production. Additionally, in patients with poor glycemic control before pregnancy, rapid improvement of HbA1c in early pregnancy can cause a temporary worsening of retinopathy, known as the early worsening phenomenon. This is thought to result from disruption of local oxygen supply-demand balance in retinal ischemic areas due to rapid glycemic improvement8).
Mechanisms of Central Serous Chorioretinopathy (CSC) During Pregnancy
Progesterone relaxes the trabecular meshwork around Schlemm’s canal, reducing intraocular pressure by facilitating aqueous humor outflow. Additionally, hemodilution due to increased circulating blood volume during pregnancy decreases blood viscosity, and changes in episcleral venous pressure also contribute to intraocular pressure reduction. In patients with normal-tension glaucoma, the decrease in intraocular pressure during pregnancy may favorably stabilize symptoms 1).
Use of anti-VEGF drugs during pregnancy:
Anti-VEGF drugs such as ranibizumab and aflibercept have shown teratogenicity in animal studies and are currently contraindicated during pregnancy. However, there are sporadic case reports of emergency use to prevent vision loss in pregnant women with proliferative diabetic retinopathy or intraocular neovascularization. Systematic data on safety are currently insufficient, and further evidence accumulation is needed 12).
Early prediction using choroidal thickness as a biomarker:
Choroidal thickness measured by OCT fluctuates during pregnancy and has been reported to change prior to the onset of preeclampsia. Research is ongoing into the potential of choroidal thickness as an early ophthalmic biomarker for preeclampsia 10).
Correlation between sFlt-1/PlGF ratio and ocular pathology:
The sFlt-1/PlGF ratio, which is becoming established as a predictive marker for preeclampsia, is being investigated for its potential correlation with the severity of fundus lesions. Observational studies have shown that cases with high ratios have a higher frequency of serous retinal detachment and Elschnig spots 5).
Standardization of glaucoma management protocols during pregnancy:
Glaucoma treatment during pregnancy currently relies on individualized approaches, and there is a need for evidence-based systematic protocols. Selective laser trabeculoplasty (SLT) may be applicable during pregnancy as an alternative to pharmacotherapy, and further investigation is expected 13).
Dinn RB, Harris A, Marcus PS. Ocular changes in pregnancy. Obstet Gynecol Surv. 2003;58(2):137-144. doi:10.1097/01.ogx.0000047741.79433.52.
Sheth BP, Mieler WF. Ocular complications of pregnancy. Current opinion in ophthalmology. 2001;12(6):455-63. doi:10.1097/00055735-200112000-00011. PMID:11734686.
Schultz KL, Birnbaum AD, Goldstein DA. Ocular disease in pregnancy. Curr Opin Ophthalmol. 2005;16(5):308-314. doi:10.1097/01.icu.0000179803.42218.cc.
Chawla S, Chaudhary T, Aggarwal S, Maiti GD, Jaiswal K, Yadav J. Ophthalmic considerations in pregnancy. Medical journal, Armed Forces India. 2013;69(3):278-84. doi:10.1016/j.mjafi.2013.03.006. PMID:24600123; PMCID:PMC3862469.
Jaffe G, Schatz H. Ocular manifestations of preeclampsia. American journal of ophthalmology. 1987;103(3 Pt 1):309-15. PMID:3826237.
Klein BEK, Moss SE, Klein R. Effect of pregnancy on progression of diabetic retinopathy. Diabetes Care. 1990;13(1):34-40. doi:10.2337/diacare.13.1.34.
Diabetes Control and Complications Trial Research Group. Effect of pregnancy on microvascular complications in the diabetes control and complications trial. The Diabetes Control and Complications Trial Research Group. Diabetes Care. 2000;23(8):1084-1091. doi:10.2337/diacare.23.8.1084.
Morrison JL, Hodgson LA, Lim LL, et al. Diabetic retinopathy in pregnancy: a review. Clin Exp Ophthalmol. 2016;44(4):321-334. doi:10.1111/ceo.12760.
Garg SJ, Federman J. Optociliary shunt vessels associated with central retinal vein occlusion and preeclampsia. Retina. 2007;27(9):1310-1311.
Ober RR, Grubman J, Engerman R, et al. The natural history of serous retinal detachment in preeclampsia. Ophthalmology. 1990;97(4):446-450.
Errera MH, Kohly RP, da Cruz L. Pregnancy-associated retinal diseases and their management. Survey of ophthalmology. 2013;58(2):127-42. doi:10.1016/j.survophthal.2012.08.001. PMID:23410822.
Mathew DJ, Pillai HJ, Demirci H. Drug safety in pregnancy and breastfeeding: ophthalmic medications. Semin Ophthalmol. 2020;35(4):237-250.
Chung CY, Kwok AK, Chung KL. Use of ophthalmic medications during pregnancy. Hong Kong medical journal = Xianggang yi xue za zhi. 2004;10(3):191-5. PMID:15181224.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.