A conjunctival laceration is a tear in the conjunctival tissue caused by external force. It is commonly seen in ophthalmic emergencies, but if a scleral laceration or globe rupture hidden beneath the conjunctival laceration is missed, it can seriously affect visual function.
Positioning under the Birmingham Eye Trauma Terminology (BETT)
Conjunctival lacerations are usually classified as superficial lacerations (lamellar laceration) in closed-globe injury. However, if there is an open scleral wound, it is an open-globe injury (open globe), so this possibility must always be kept in mind during examination.
The main injury mechanisms for conjunctival laceration are as follows.
Sports injuries: Blows from balls, elbows, or fingers are common. The frequency of eyelid conjunctival injury in sports-related eye trauma is as high as 28%.
Falls and collisions: Playground accidents and falls in children, and falls in older adults.
Traffic accidents: Direct trauma from vehicle interior structures or flying debris.
Sharp injuries: Cuts from glass fragments, metal fragments, tree branches, or fingernails.
Occupational injuries: Injuries from flying debris and tools in manufacturing and construction.
The incidence of severe eye trauma in children is 11.8 per 100,000 people per year, and children make up at least 35% of severe eye trauma cases, many of them under 12 years old. Trauma is the leading cause of blindness in one eye in children, and even when the injury looks minor, internal damage may be present.
QCan a conjunctival laceration heal without stitches?
A
Small conjunctival lacerations (about less than 1 cm) often heal on their own in 3 to 5 days with antibiotic eye drops alone. Larger lacerations (1 cm or more) or lacerations with widely separated edges need suturing with 8-0 to 9-0 absorbable sutures. However, regardless of whether suturing is needed, the first priority is to check whether a scleral laceration or globe rupture is hidden beneath the conjunctival laceration.
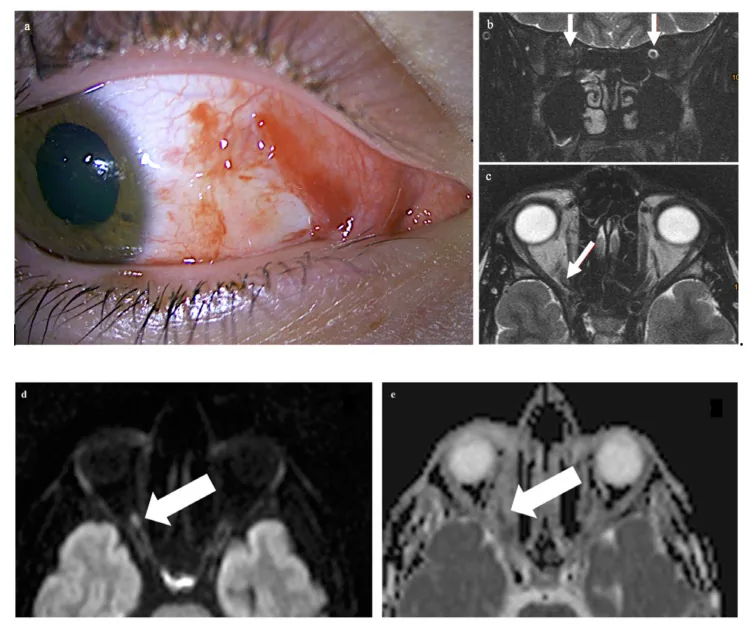
Stahl A, Hosten N. Trauma to the Eye: Diffusion Restriction on MRI as a Surrogate Marker for Blindness. Tomography. 2023;9(1):413-419. Figure 1(a). PMID: 36828385. PMCID: PMC9968198. License: CC BY 4.0.
Post-injury anterior segment clinical photograph (panel a) showing a superficial conjunctival laceration (conjunctival wound) and subconjunctival hemorrhage on the nasal side of the right eye, with mydriasis. This corresponds to the clinical findings of conjunctival laceration and subconjunctival hemorrhage discussed in the section “Main symptoms and clinical findings”.
A particularly important point is when a globe rupture is hidden beneath the conjunctiva. If severe conjunctival bleeding makes the sclera hard to see, it may be covering a globe rupture. A combination of severe 360-degree conjunctival bleeding, low eye pressure, and a distorted pupil strongly suggests an occult globe rupture and requires urgent evaluation.
Also watch for hyphema. This is a condition in which blood collects in the anterior chamber after an injury, and it suggests reduced vision, increased eye pressure, or damage to structures inside the eye.
QIs it okay if only the white of the eye is red?
A
Conjunctival bleeding after an injury may be a simple subconjunctival hemorrhage, but a scleral tear or globe rupture may be hidden underneath. In particular, if there is 360-degree bleeding, low eye pressure (the eye feels soft), a distorted or fixed pupil, or prolapse of intraocular contents, urgent evaluation is needed. With redness or bleeding after an injury, you should always see an ophthalmologist to rule out occult globe rupture.
In blunt trauma, the impact on the eye causes a rapid rise in intraocular pressure, and rupture is more likely to occur at the thinnest parts of the eye (near the limbus or upper sclera, for example). In sports-related eye injuries, the most common injuries are anterior segment injuries (72%), while the conjunctiva and eyelids are injured in 28%.
Ball sports: baseball, softball, tennis, badminton, and more. The higher the ball speed, the more severe the injury.
Combat and contact sports: boxing, judo, rugby, and more. Blows from fists and elbows are common.
Falls and collisions: bicycle or skateboard accidents, collisions with stairs or the corner of a table, and more.
Traffic accidents: airbag deployment, shattered windshield, impact against the steering wheel.
In direct trauma from a sharp object, the injury site is clear and it is relatively easy to assess how deep the wound is, but it is important to check for a retained intraocular foreign body.
Glass fragments and metal fragments: debris scattered during work. They may remain as intraocular foreign bodies.
Tree branches and plant thorns: organic foreign bodies with a high risk of infection. Some materials are difficult to detect on CT or MRI.
Fingernails, stationery, and cooking utensils: direct injuries from everyday items.
Knives and scissors: sharp cuts that are often associated with deep injury.
In children, the cause and situation of injury are different from those in adults. Injuries often happen from playground accidents, contact while playing tag, pointed toys, or pencils. Because children are uncooperative, examination can be difficult and the injury may be underestimated. The possibility of abuse also needs to be kept in mind during the examination.
Fluorescein staining helps confirm the extent of the epithelial defect and is useful for avoiding missed small perforating wounds.
Seidel test: fluorescein is applied and observed under cobalt blue light. If aqueous humor is leaking from the eye, the fluorescein is diluted in a streaming pattern and shows a positive finding, confirming an open-globe injury (perforation or laceration). Small perforations may still be negative, so if in doubt, prioritize examination in the operating room.
Used to assess the laceration in detail (width, length, depth, and whether the sclera is exposed) and to check anterior chamber depth, inflammation, and bleeding. If the anterior chamber is shallow or absent, strongly suspect an open-globe injury.
If open-globe injury (scleral laceration or globe rupture) is suspected, measuring intraocular pressure is contraindicated because it compresses the eye. Limit evaluation to a simple finger palpation over the eyelids with two index fingers. A low pressure feeling (soft, mushy) is a strong sign suggesting globe rupture.
If a metallic intraocular foreign body is suspected, obtain CT (thin slices). For nonmetallic foreign bodies (wood, plastic), CT may be difficult to show, and MRI (T1-weighted) can sometimes be useful, but only after metallic foreign body has been ruled out.
Mechanism of injury (high-speed flying debris), CT, and confirmation of the entry wound on slit-lamp microscopy
QCan intraocular pressure be measured in a conjunctival laceration?
A
If an open injury (scleral laceration or globe rupture) is suspected, it is contraindicated because applying the tonometer can press on the eye. Limit assessment to a gentle finger palpation method through the eyelid to check firmness. If hypotony is suspected or the diagnosis cannot be confirmed on examination, prioritize imaging and detailed examination in the operating room.
Small conjunctival lacerations under about 1 cm often do not need sutures and usually heal on their own within 3 to 5 days with the following conservative treatment.
Antibiotic eye drops: Instill a broad-spectrum antibiotic such as levofloxacin 1.5% eye drops 4 times a day.
Follow-up: Return after 3 to 5 days to confirm healing.
Eye patch: Use if needed, but avoid a patch that presses on the eye until an open injury has been ruled out.
Management of small lacerations (under 1 cm)
Antibiotic eye drops only: Levofloxacin 1.5%, etc., 4 times a day
No sutures needed: Heal naturally if the edges are in contact
Observation period: Confirm healing in 3 to 5 days
Recheck: Consider suturing if healing is poor or there are signs of infection
Management of large lacerations and associated injuries
Conjunctival suturing: 8-0 or 9-0 polyglactin 910 (absorbable suture)
With scleral injury: Scleral suturing in the operating room (7-0 to 8-0 nylon suture)
Consider general anesthesia: when the patient is a child or swelling and bleeding make it hard to see
Open injury: prepare for urgent surgery, avoid pressure, and apply a protective eye shield
If a scleral laceration is suspected, examination and suturing in the operating room (clean environment, good lighting, magnified view) are essential.
Scleral suturing: close with 7-0 to 8-0 nylon sutures (nonabsorbable).
Consider general anesthesia: if it is difficult to confirm the laceration in a child or because of swelling and bleeding, consider treatment under general anesthesia.
Infection prevention: Use broad-spectrum antibiotics as eye drops and systemic treatment (intravenous infusion). This is especially important to prevent endophthalmitis.
Emergency response for prolapsed intraocular contents and globe rupture
If prolapse of intraocular contents (such as the uvea) is confirmed, prioritize the following steps.
Avoid pressure: Do not do anything that puts pressure on the eye (including measuring eye pressure or applying excessive pressure with an eye patch).
Apply a protective eye shield: Use a Fox shield–type protective eye shield that does not touch the eyeball.
Pain relief, sedation, and antiemetics: These help prevent worsening of the prolapse caused by increased eye pressure from vomiting.
Nothing by mouth: In preparation for surgery (general anesthesia).
Emergency open wound closure surgery: Perform surgical closure promptly to reduce the risk of endophthalmitis.
QMy child hit their eye. Should we go to an eye doctor right away?
A
If symptoms such as redness, bleeding, constant tearing, or inability to open the eye occur after hitting the eye, an eye doctor should be seen promptly. Trauma is the leading cause of blindness in one eye in children, and even when it looks mild, there may be damage inside the eyeball. Urgent care is especially needed if the eyeball feels soft, the pupil looks misshapen, or the white of the eye is heavily bleeding.
This is the mechanism in which a sharp object directly cuts the conjunctiva. The site of injury is clear, and the laceration usually has a straight or simply irregular shape. The depth varies depending on the object’s shape, speed, and angle, ranging from a superficial tear to a full-thickness injury (scleral exposure or perforation). Organic foreign bodies (wood splinters, plants) carry a high risk of infection, and attention is needed for endophthalmitis caused by soil bacteria such as Bacillus species.
Impact to the eyeball causes a sudden rise in intraocular pressure, leading to laceration or rupture at the thinnest and weakest part of the eye wall. Blunt trauma has the following features:
Fragility near the limbus: The limbus, where the sclera and cornea meet, is structurally thin and prone to laceration or rupture with blunt trauma.
Elasticity of the conjunctiva: Because the conjunctiva is highly elastic, the underlying sclera may be torn even when the conjunctiva itself is intact in blunt trauma. This is a main mechanism behind a hidden globe rupture.
Spread to the posterior part of the eyeball: A blow to the front can cause a sudden rise in intraocular pressure, and rupture may also occur at thin areas of the posterior sclera (such as around the lamina cribrosa).
Lacerations near the inner corner of the eye and canalicular rupture
With conjunctival lacerations near the inner corner of the eye (medial canthus), associated canalicular rupture must be considered. The canaliculus lies just beneath the conjunctiva and can be torn by direct or indirect traction. Rupture of the lower canaliculus is especially common, and if missed, it can cause chronic tearing (overflowing tears).
Simple conjunctival laceration: Good prognosis. With proper treatment, it usually heals within 1 to 2 weeks.
With scleral laceration: Prognosis is relatively good if the sclera is closed properly, but there is a risk of endophthalmitis.
With globe rupture: Visual prognosis is often poor. In particular, the initial visual acuity, intraocular pressure, and whether intraocular contents have prolapsed affect the prognosis. It may also be accompanied by injuries with no treatment, such as choroidal rupture and retinal contusion necrosis, and sometimes observation or delayed surgery must be considered.
Epidemiologic studies are progressing on the incidence and injury patterns of eye trauma by sport. Reports are accumulating that mandating protective eyewear with polycarbonate lenses can greatly reduce sports-related eye injuries. Widespread use of protective eyewear in sports organizations and school sports is a future challenge.
Using anterior segment optical coherence tomography (anterior segment OCT) may make it possible to noninvasively evaluate the layered structure of the conjunctiva and sclera. Its use for ruling out open injuries and monitoring the healing process is expected.
After eye trauma in children, there is a risk of developing amblyopia (impaired visual development). Research is under way on long-term follow-up of vision after injury and on the appropriate timing for starting amblyopia treatment (such as occlusion therapy).
Zhou Y, DiSclafani M, Jeang L, Shah AA. Open Globe Injuries: Review of Evaluation, Management, and Surgical Pearls.Clin Ophthalmol. 2022;16:2545-2559. PMID: 35983163. PMCID: PMC9379121. (PMC)
開放性眼球損傷の評価・管理・手術手技を包括的にレビュー。Seidel試験・眼圧測定の禁忌・前房評価・受傷後12〜24時間以内の早期閉鎖の重要性を解説しており、結膜裂傷の下に隠れた強膜裂傷・眼球破裂の除外と緊急手術判断の根拠として参照した。
Ohana O, Alabiad C. Ocular related sports injuries.J Craniofac Surg. 2021;32(4):1606-1611. PMID: 33741878. PMCID: PMC8192440. (PMC)
米国で年間4万件超のスポーツ関連眼外傷が発生し、その90%はポリカーボネート製保護眼鏡(通常眼鏡の20倍の保護効果)の着用で予防可能であることを報告。本記事におけるスポーツ眼外傷の予防と保護眼鏡推奨の根拠とした。
Chaudhary A, Carr EW, Bogan F, Liu JX, Hajrasouliha AR. An Analysis of Ocular Trauma Resulting From Pediatric Sports Injuries.Clin Ophthalmol. 2025;19:507-517. PMID: 39963522. PMCID: PMC11831506. (PMC)
小児スポーツ眼外傷1,290例の10年間レトロスペクティブ研究。野球(38.5%)・バスケットボール(16.9%)・サッカー(14.9%)が主要原因で、約90%が予防可能と結論。年齢別の受傷機転(年少児では野球、年長児ではサッカー・フットボール)の記述根拠とした。
Al-Battashy A, Al-Mujaini AS. Canalicular lacerations: Techniques used and timing to intervene.Oman J Ophthalmol. 2023;16(2):201-204. PMID: 37602159. PMCID: PMC10433052. (PMC)
涙小管裂傷は眼瞼裂傷の16〜20%に合併し、内眼角付近の結膜裂傷で見逃すと慢性流涙の原因となる。顕微鏡下縫合(gold standard)と早期修復の重要性を示しており、本記事の「内眼角付近の裂傷と涙小管断裂」の項の根拠とした。
Stahl A, Hosten N. Trauma to the Eye: Diffusion Restriction on MRI as a Surrogate Marker for Blindness.Tomography. 2023;9(1):413-419. PMID: 36828385. PMCID: PMC9968198. (PMC)
穿通性眼外傷後の視神経損傷をMRI拡散強調像で評価した症例報告。視診で完全評価が困難な開放性外傷における画像検査の補助的役割を示しており、本記事の「画像検査」の項および臨床写真(Figure 1a, CC BY 4.0)の引用元とした。
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.