A conjunctival foreign body is a state in which a foreign body sticks to or enters the upper and lower tarsal conjunctiva, bulbar conjunctiva, or fornix conjunctiva. It accounts for 4.4% of new ophthalmology outpatients, and 75% are men. Unlike a corneal foreign body, the conjunctiva is relatively less sensitive to pain, and especially in the fornix, even large foreign bodies may cause only mild symptoms.
The average size of a conjunctival foreign body is 0.52 mm long, 0.34 mm wide, and 0.25 mm thick. Foreign bodies thicker than 0.5 mm are often lifted by tears and naturally washed out with blinking.
urticating hairs (from poisonous caterpillars, cocoons, and shed skins)
3%
stellate hairs (hairs from plant leaves and stems)
0.4%
Most are tiny inorganic or organic foreign bodies such as wood chips, iron, and sand. Urticating hairs are less common at 3%, but if they remain, they can cause serious complications. Stellate hairs (the hairs on plant leaves and stems) are the rarest at 0.4%, but they can cause ophthalmia nodosa.
QWhat should I do first if something gets in my eye?
A
First, the most important thing is not to rub the eye. Rubbing can scratch the cornea and may move the foreign body to the upper tarsal conjunctiva or the fornix. Rinse the eye with clean water or try to gently remove it with a damp cotton swab. If it does not come out or the pain continues, see an eye doctor. Avoid forceful removal because it can injure the cornea.
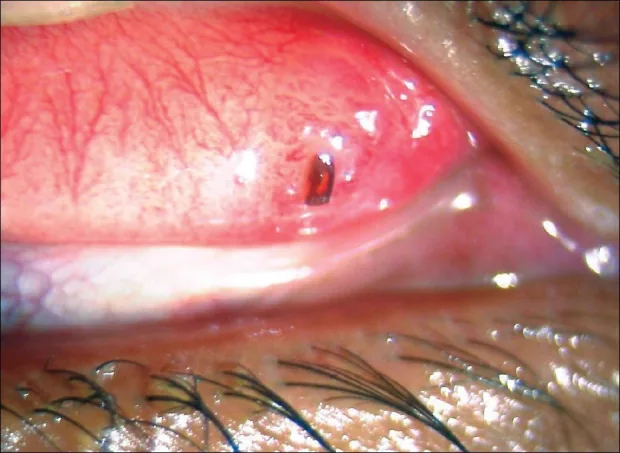
Babu K, Maralihalli RE. Insect wing tarsal foreign body causing conjunctival granuloma and marginal keratitis. Indian J Ophthalmol. 2009;57(6):473-474. Figure 2. PMID: 19861755. PMCID: PMC2812772. License: CC BY.
A black insect wing fragment is embedded in the upper tarsal conjunctiva exposed by upper eyelid eversion, with a raised conjunctival granuloma forming around it. This corresponds to the finding described in the section “2. Main symptoms and clinical findings” for confirming a foreign body in the upper tarsal conjunctiva by upper eyelid eversion.
The main symptoms are eye pain, foreign-body sensation, and tearing. When a thorny grass seed or awn becomes embedded, the pain can be severe. The fornix has reduced sensation, so even a large foreign body may cause only mild symptoms.
If fluorescein staining shows a corneal abrasion, a foreign body is often present on the opposing conjunctival surface.
Symptoms of a typical conjunctival foreign body
Eye pain and foreign-body sensation: These appear soon after the object enters. The severity depends on the size and shape of the foreign body.
Tearing: Reflex tearing is marked, with repeated blinking.
Fornix foreign body: Because sensation is reduced, even a large foreign body may cause relatively few symptoms.
Corneal abrasion: Linear staining is seen with fluorescein staining. A foreign body is present on the opposing conjunctival side.
Findings suggesting stinging hairs
Linear corneal epithelial defects: Numerous fine linear epithelial defects are detected with fluorescein.
Severe eye pain: Persistent, intense pain continues because of irritation from the barbed stinging hairs.
Foreign-body furrows and black hairs on the lower tarsal conjunctiva: Black hairs about 0.03 mm thick and 0.5–1.5 mm long are seen.
Not relieved by rinsing: Stinging hairs do not dissolve in water, acid, or alkali, so they cannot be removed by rinsing the eye.
QHow do stinging hairs get into the eye?
A
The stinging hairs of toxic caterpillars (チャドクガ・マッカレハ・ヒロヘリアオイラガ, etc.) can also fall from shed skins and cocoons. They may be carried by the wind, stick to laundry, or get into the eye during pruning of garden trees. Because they are extremely thin at 0.03 mm, you may not notice when they enter.
In outdoor work (farming, forestry, and gardening), wood chips, straw, and plant fragments often scatter. In metalworking and construction, injuries from iron filings and metal fragments are common. In daily life, sand, pebbles, ash, and charcoal can also get into the eye. Scrub soap may let particles enter the eye while washing the face.
The stinging hairs of toxic caterpillars reach the eye through the following routes.
Cha-dokuga (often lives on the undersides of camellia and sasanqua leaves)
Maccareha (parasites on plants in the rose family)
Hirohera-aoiraga (parasites on oak and sawtooth oak trees, etc.)
Even without direct contact with the caterpillar itself, the hairs can enter the eye indirectly through shed skins, cocoons, or laundry. The risk is especially high during caterpillar season (spring to summer).
Stellate hairs come from plants (the hairs on plant leaves and stems, not from caterpillars). If they enter the conjunctiva, they can cause granulomatous inflammation (ophthalmia nodosa). The frequency is low at 0.4%, but they are difficult to detect with a slit-lamp microscope alone, and fluorescein staining is essential.
It is difficult to detect stinging hairs or tiny transparent debris embedded in the upper tarsal conjunctiva with slit-lamp microscopy alone. Fluorescein eye drops should always be used to avoid missing them. Corneal abrasion marks that stain with fluorescein suggest the presence of a foreign body, and the foreign body is often on the opposite side.
Upper eyelid eversion (turning the eyelid inside out)
Fifty-eight percent of conjunctival foreign bodies are found in the upper tarsal conjunctiva. Without upper eyelid eversion, more than half may be missed. Eversion of the upper eyelid to inspect the entire tarsal conjunctiva and superior fornix is an essential procedure1. Foreign bodies left in the tarsal conjunctiva for a long time have been reported to cause conjunctival granuloma and marginal keratitis2.
Detailed examination when stinging hairs are suspected
If a stinging hair is found in the conjunctival sac, a detailed examination of the retina and vitreous is needed to rule out penetration into the vitreous body. Stinging hairs do not dissolve in water, acid, or alkali, and their barbs on the surface let them move forward through tissue in one direction, so they may have reached the vitreous body34.
Stinging-hair granuloma (ophthalmia nodosa): Granulomatous inflammation caused by stinging hairs. It may also extend to the cornea and uvea.
QHow do you examine the inside of the upper eyelid?
A
The upper eyelid is turned inside out using a procedure called upper eyelid eversion. Since 58% of conjunctival foreign bodies are in the upper tarsal conjunctiva, they may be missed without this procedure. It is a standard examination technique performed by ophthalmologists. The patient is asked to look downward, and the skin of the upper eyelid is pulled outward as it is turned inside out.
Most conjunctival foreign bodies can be removed without topical anesthesia by rubbing them off with the corner of a piece of moistened cotton folded into eight layers. When the cotton is unfolded, the foreign body remains in the center, so it can be shown to the patient and used for informed consent.
For iron filings, after topical anesthesia, remove them with a foreign body needle. Scrape off the settled rust with the tip of the foreign body needle.
Method for removing common foreign bodies
Topical anesthesia: generally not needed.
Instrument: moistened cotton (folded into eight layers and use the corner).
Procedure: Rub the foreign body off with the corner of the moistened cotton. The unfolded cotton can be shown to the patient to support informed consent.
For iron filings: After topical anesthesia, remove with a foreign body needle. Scrape off the rust with the tip of the foreign body needle.
Method for removing stinging hairs
Topical anesthesia: required.
Instrument: non-toothed forceps.
Procedure: Grasp the exposed base and gently pull it out.
Notes by type: Makkareha is easy to remove. Hiroheria Oiraga has sharp, hooked barbs that break easily, so it is scraped out while making an incision with a foreign-body needle. Stinging hairs under the bulbar conjunctiva can enter the eye, so complete removal is essential.
After topical anesthetic eye drops, ask the patient to look downward, then evert the upper eyelid and press it slightly, and part of the foreign body will appear. For spiny foreign bodies such as grass awns, grasp the exposed end with non-toothed forceps and pull it out in the same direction it entered, without pulling against the spines.
After foreign body removal, in every case evert the eyelid, wash away fluorescein and any remaining conjunctival foreign body, and apply antibiotic eye ointment. If an incision was made when removing the foreign body, arrange follow-up and prescribe antibiotic eye drops (three times a day) and antibiotic eye ointment (before bedtime).
QWhat happens if caterpillar stinging hairs remain in the eye?
A
Because of their barbed structure, stinging hairs move in one direction through tissue. They travel from the conjunctiva to the sclera and then toward the vitreous, and once they reach the vitreous they can cause severe uveitis over the course of several years. If stinging hairs are found in the conjunctival sac, a retinal-vitreous examination and complete removal are necessary.
6. Pathophysiology and detailed mechanism of onset
When a foreign body enters the eye, pain triggers heavy tearing and blinking. Foreign bodies 0.5 mm or larger are lifted by tears and swept out with blinking. Rubbing the eye can move a large foreign body into the fornix.
Among foreign bodies left on the corneal surface, those with a rough surface move to the tarsal conjunctiva and become fixed there. Round foreign bodies settle in the foreign-body groove between the tarsal conjunctiva and the eyeball. This leads to the observed distribution of 58% in the upper tarsal conjunctiva and 23% in the foreign-body groove.
The special features of stinging hairs can be summed up in three points.
Chemical insolubility: They do not dissolve in water, acid, or alkali. Chemical removal with eye washing or solutions is not possible.
Physical forward movement: The surface has countless barbs pointing opposite to the tip. With each movement of the eyelid or eyeball, the barbs catch in the tissue and move forward in one direction (front to back).
Tissue penetration: They move in the direction of the conjunctiva -> sclera -> vitreous -> retina. Stinging hairs that enter the vitreous cause severe uveitis (caterpillar-induced ophthalmia) over several years45.
This mechanism of one-way forward movement explains the clinical course in which stinging hairs that were in the conjunctiva when first found are discovered years later in the vitreous3. In recent years, an observational study that followed the clinical course for up to one year has also been reported for eye injury caused by the stinging hairs of the oak processionary caterpillar6.
When stellate hairs (tiny plant hairs) enter the conjunctiva, a granuloma forms around the foreign body (ophthalmia nodosa). The granuloma can extend to the cornea, iris, and vitreous, and chronic inflammation may continue. Because they are transparent and tiny, they are hard to find with slit-lamp microscopy alone, and fluorescein staining is essential for diagnosis.
Case reports of caterpillar-induced ophthalmia have accumulated from around the world, but systematic treatment guidelines and evidence-based prognosis data are still limited. Research is underway on the indications for and timing of vitrectomy for stinging hairs that remain in the vitreous cavity or move within it.
Classification and management of eye damage caused by plant hairs
Standardization of the severity classification for ophthalmia nodosa (conjunctival, corneal, uveal, and panophthalmic types) is being discussed internationally. In particular, consensus is needed on the indications for and methods of surgical management of stellate hairs in the cornea and anterior chamber.
Noninvasive alternative test to upper eyelid eversion
Upper eyelid eversion is currently the standard procedure for diagnosing foreign bodies, but it requires skill and can be uncomfortable for patients. A non-contact method for observing the upper tarsal conjunctiva using anterior segment OCT is being explored.
Stevens S. Ophthalmic practice. Community Eye Health. 2005;18(55):109-110. PMID: 17491771. PMCID: PMC1705681. ↩
Babu K, Maralihalli REY. Insect wing tarsal foreign body causing conjunctival granuloma and marginal keratitis. Indian J Ophthalmol. 2009;57(6):473-474. PMID: 19861755. PMCID: PMC2812772. ↩
Ascher KW. Mechanism of locomotion observed on caterpillar hairs. Br J Ophthalmol. 1968;52(2):210. PMID: 5300404. PMCID: PMC506555. ↩↩2
Joshi D. Ophthalmia nodosa with intraocular caterpillar setae. Med J Armed Forces India. 2011;67(2):167-168. PMID: 27365792. PMCID: PMC4920753. ↩↩2
Al Somali AI, Otaif W, Afifi TM, et al. Ophthalmia nodosa secondary to multiple intraocular caterpillar hairs in a 2-year-old girl. Saudi J Ophthalmol. 2021;34(3):230-232. PMID: 34085024. PMCID: PMC8081091. ↩
Leclaire MD, Vietmeier FE, Treder M, Eter N, Baydoun L. Ocular involvement of oak processionary caterpillar hairs: Clinical outcome up to one year. Graefes Arch Clin Exp Ophthalmol. 2024;263:771-779. PMID: 39532718. PMCID: PMC11953161. ↩
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.