Conjunctival prolapse (Conjunctival Prolapse) is when the bulbar conjunctiva or fornix conjunctiva moves out of its normal position and protrudes beyond the eyelid margin.
Normally, the bulbar conjunctiva is loosely attached to Tenon’s capsule and the surface of the sclera, and it stays within the palpebral fissure. When this attachment is lost for some reason, or when the conjunctival tissue becomes lax or excessive, it can protrude beyond the eyelid margin.
It is broadly divided into acute and chronic forms depending on how it starts. The acute form develops after eye trauma or surgery, and the conjunctiva suddenly prolapses. The chronic form occurs when age-related conjunctival laxity has progressed severely (a severe form of conjunctivochalasis) and worsens gradually.
This is a relatively rare condition, but it may be encountered during emergency care after eye trauma or during postoperative follow-up. Early, accurate diagnosis and evaluation of the cause are key to management.
QHow is conjunctival prolapse different from conjunctival edema (chemosis)?
A
Conjunctival edema (chemosis) is a state in which fluid collects within conjunctival tissue due to allergy, infection, trauma, or other causes, causing the conjunctiva to swell into a translucent, boggy mass. A characteristic feature is that it indents when pressed. By contrast, conjunctival prolapse is a state in which the conjunctival tissue itself physically protrudes beyond the eyelid margin and feels more solid. Severe chemosis can worsen and progress to conjunctival prolapse. To distinguish the two, assess the transparency of the conjunctiva, whether it deforms with pressure, and the mobility of the prolapsed tissue.
Gzzz. Chemosis due to allergy to pollens. Wikimedia Commons. 2016. Source ID: commons:File:Chemosis_(1).jpg. License: CC BY-SA 4.0.
Clinical appearance of chemosis due to pollen allergy, in which the bulbar conjunctiva bulges translucently beyond the lower eyelid margin and protrudes outside the eyelid. Corresponds to conjunctival edema (chemosis) and conjunctival prolapse discussed in the section ‘2. Main symptoms and classification’ of the text.
Mild: The conjunctiva protrudes slightly beyond the eyelid margin. It can be put back naturally or with gentle pressure.
Moderate: The conjunctiva clearly prolapses outside the eyelid. Manual repositioning is possible, but it tends to prolapse again.
Severe: A large amount of conjunctiva prolapses, and the exposed conjunctiva is at risk of drying out and necrosis. Surgical repositioning is needed.
QA white, membrane-like tissue is coming out of my eye. What should I do?
A
This may be conjunctival prolapse. Do not try to push it back in with clean hands; it is important to see an ophthalmologist as soon as possible. Especially if it occurred after an injury, there may be a perforation of the eyeball (penetration into the eye), so urgent care is needed. Until you are seen, lightly cover the conjunctiva with clean moist gauze to keep it from drying out.
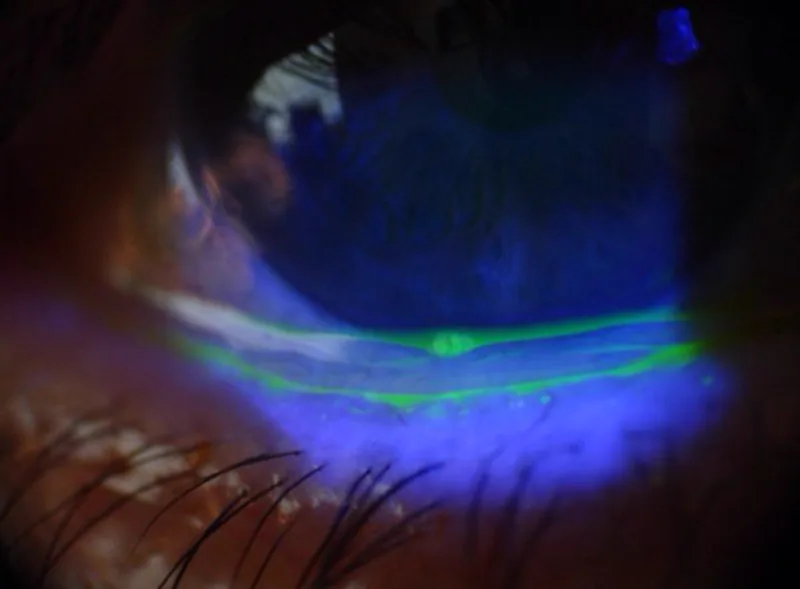
Dalianis G, Trivli A, Terzidou C, et al. The Location of Conjunctivochalasis and Its Clinical Correlation with the Severity of Dry Eye Symptoms. Medicines (Basel). 2018;5(1):12. Figure 2. DOI: 10.3390/medicines5010012. License: CC BY 4.0.
In a slit-lamp image under fluorescein staining, excess conjunctival folds are seen as green fluorescence along the inferior limbus. This corresponds to severe conjunctivochalasis covered in the section “3. Epidemiology and Causes”.
Data on the exact prevalence and incidence are limited. It has been reported as a relatively rare condition in the fields of oculoplastic surgery and emergency ophthalmology.
Post-traumatic conjunctival prolapse can occur as a complication of perforating eye injuries and blunt eye injuries. In globe rupture, the bulbar conjunctiva can tear, and the conjunctiva may prolapse along with the eye contents. It is often seen after high-energy trauma such as explosions, traffic injuries, and sports injuries.
Postoperative conjunctival prolapse can occur after the following surgeries.
Strabismus surgery (dehiscence of the conjunctival incision or suture line)
Pterygium surgery (tissue shortage after extensive conjunctival excision)
Glaucoma filtering surgery (laxity and fragility of the conjunctiva around the bleb)
After orbital surgery or enucleation (due to changes in the orbital tissues)
Severe conjunctivochalasis occurs when, with aging, the attachment between the conjunctival tissue and Tenon’s capsule loosens, leading to excessive conjunctival folds; in severe cases, this can result in prolapse outside the eyelid. Risk factors include older age, dry eye, and chronic eyelid irritation (such as rubbing during sleep).
Thyroid eye disease (Graves’ ophthalmopathy) and other diseases that cause proptosis can push the conjunctiva outward beyond the eyelid because of increased orbital pressure and forward displacement of the eyeball. In such cases, chemosis and conjunctival prolapse often occur together.
Confirm by visual inspection whether conjunctival tissue has prolapsed beyond the eyelid margin. During the examination, assess the following:
Amount and location of the prolapsed conjunctiva (upper, lower, or circumferential)
Conjunctival color (whether there is redness, necrosis, or dryness)
Relationship with the eyelid (whether it is trapped)
Presence of perforation (highest priority after trauma): check for low intraocular pressure, iris prolapse, and vitreous prolapse.
Assessment of the underlying cause: history of trauma, surgery, thyroid disease, and conjunctival laxity.
Fluorescein staining is used to assess the degree of epithelial damage in exposed conjunctiva and cornea. Detailed anterior segment examination with a slit lamp microscope is the basis.
Manual reduction: Gently reposition the conjunctiva with a clean cotton swab or a moistened sterile cotton swab.
Pressure bandage (patching): After reduction, apply a pressure bandage to the eye to prevent it from prolapsing again. It is usually worn for 24 to 48 hours.
Eye drops: Use a combination of antibiotic eye drops (to prevent infection), steroid eye drops (to reduce inflammation and swelling), and artificial tears (to prevent dryness of exposed conjunctiva and cornea).
Surgical treatment (severe or recurrent)
Conjunctival excision and suturing: Remove the excess conjunctiva and suture the cut edges to reposition it.
Conjunctival pexy: Suture the conjunctiva to the sclera to prevent it from prolapsing again.
Tenon’s capsule repair: If Tenon’s capsule is markedly weakened, repair it at the same time.
The pressure bandage is usually kept on for 24–48 hours, then reassessed. In mild cases, spontaneous reduction may be maintained after the pressure bandage is removed.
Emergency treatment for post-traumatic conjunctival prolapse
In mild cases, manual repositioning, pressure bandaging, and eye drops may help maintain spontaneous reduction. However, in moderate or more severe cases, or when it recurs, conservative treatment alone is not enough and surgical treatment (conjunctival resection and suturing, or conjunctival fixation) is needed. If the cause is thyroid eye disease or severe conjunctivochalasis, treating the underlying condition leads to the fundamental solution. In any case, early ophthalmology consultation is important.
6. Pathophysiology and detailed mechanism of onset
Bulbar conjunctiva is a thin mucosal tissue that covers the surface of the eye (from the limbus to the fornix), and its deep layer is loosely attached to the sclera via Tenon’s capsule (ocular fascia). At the fornix, it transitions to the palpebral conjunctiva and lines the eyelids. Normally, it stays within the palpebral fissure and does not prolapse beyond the eyelid margin.
After trauma or surgery:
When ocular trauma or surgical manipulation disrupts the continuity of the conjunctiva, the attachment to Tenon’s capsule and the scleral surface is lost. Movement of the eyelids and eyeball pulls the conjunctival edge out beyond the eyelid, causing prolapse. After penetrating trauma in particular, sudden changes in intraocular pressure promote tearing of the conjunctiva and Tenon’s capsule.
Increased orbital pressure:
Edema and fibrosis of orbital fat and extraocular muscles in thyroid eye disease, or increased orbital pressure from an orbital tumor, push the eyeball forward. With this forward displacement, the eyelids can no longer fully cover the eye, and the conjunctiva protrudes from the eyelid margin.
Age-related conjunctival laxity:
With aging, collagen and elastin in Tenon’s capsule and the conjunctival stroma degenerate, loosening the attachment between the conjunctiva and Tenon’s capsule. Excess conjunctival tissue (a lax, redundant fold) forms and protrudes beyond the eyelid because of gravity and the physical pressure of the eyelids. Friction from the eyelids during sleep is thought to accelerate this process.
Weakening of Tenon’s capsule:
If Tenon’s capsule, the main supporting structure of the conjunctiva, becomes weakened by surgery, inflammation, or aging, it can no longer keep the conjunctiva in its normal position. In cases where extensive dissection of Tenon’s capsule has been performed, such as after glaucoma filtering surgery, the risk of postoperative conjunctival laxity and prolapse increases.
The prolapsed conjunctiva is directly exposed to air, causing dryness and epithelial damage. If mechanical irritation from the eyelids (pinching) is repeated, redness and swelling worsen. If left for a long time, the prolapsed conjunctiva may become necrotic, leading to irreversible tissue damage, so early treatment is needed.
Comparison of surgical techniques for conjunctival laxity:
Reports have compared conjunctival cauterization (thermal coagulation), conjunctival excision and suturing, and conjunctival fixation procedures (including Tenon capsule fixation) as techniques for severe conjunctival laxity. In the literature review by Meller & Tseng, excessive production of collagen fibers and increased metalloproteinase activity in the conjunctival epithelium were suggested as possible factors in the pathophysiology of conjunctival laxity1).
Compression suturing for severe chemosis:
For severe chemosis and conjunctival prolapse after thyroid eye disease or orbital surgery, temporary tarsorrhaphy or conjunctival suturing to the eyelids has been reported to be effective. Evaluation of long-term outcomes, including effects on tear volume and eyelid function, remains an issue2).
Conjunctival management after orbital decompression:
After orbital decompression for thyroid eye disease, techniques to secure the conjunctiva during surgery have been reported to help prevent conjunctival laxity and prolapse. Establishing a standard preventive protocol remains a future task.
Establishing standard classification and treatment algorithms:
A unified severity classification and treatment algorithm for conjunctival prolapse has not yet been established. Standardization through multicenter collaborative research in the oculoplastic surgery field is needed.
Meller D, Tseng SC. Conjunctivochalasis: literature review and possible pathophysiology. Surv Ophthalmol. 1998;43(3):225-232.
Watanabe A, Selva D, Kakizaki H, et al. Long-term tear volume changes after blepharoptosis surgery and blepharoplasty. Invest Ophthalmol Vis Sci. 2015;56(1):54-58.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.