Optic nerve avulsion (ONA) is a condition in which the optic nerve is separated from the eye at the level of the lamina cribrosa due to trauma. It is also called optic nerve head avulsion and refers to the same condition. It is not accompanied by rupture of the optic nerve dural sheath or adjacent sclera1).
In optic nerve avulsion, the continuity of the optic nerve dura is maintained, and the nerve fibers rupture at the structurally weak, unmyelinated portion of the lamina cribrosa. Optic nerve evulsion and optic nerve avulsion refer to the same condition but are distinguished etymologically.
Optic nerve avulsion is a type of traumatic optic neuropathy (TON) and is classified as anterior traumatic optic neuropathy1). Traumatic optic neuropathy overall occurs in 0.5–5% of head injuries 5), and optic nerve avulsion is a rare subtype 2). It ranges from partial to complete avulsion and can have devastating effects on visual function 1).
The most common sites of avulsion are the optic nerve head (most frequent), orbital apex, and optic chiasm1). The most common cause is traffic accidents, followed by sports injuries, falls, and fights. In a meta-analysis by Buchwald et al., small blunt objects or fingers accounted for 49% of causes 1). Optic nerve avulsion occurs especially when a strong rotational force is applied, such as when a finger enters the orbit. It is recognized as a rare but severe injury in blunt ocular trauma associated with boxing, traffic accidents, and sports.
QWhat is the difference between optic nerve avulsion (optic nerve head avulsion) and traumatic optic neuropathy (TON)?
A
Optic nerve avulsion is a type of traumatic optic neuropathy, referring to physical separation at the level of the lamina cribrosa. Traumatic optic neuropathy encompasses a broad spectrum from contusion to complete transection, and optic nerve avulsion is considered one of the most severe forms 1).
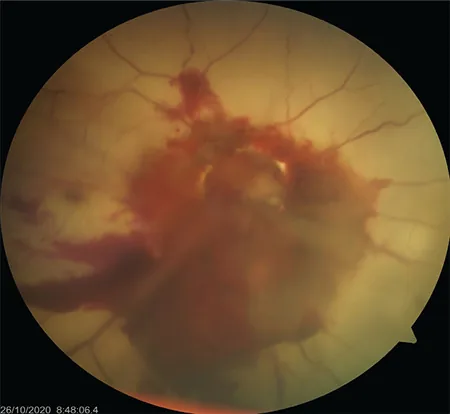
Mahjoub A, Sellem I, Mahjoub A, et al. Optic nerve avulsion: Case report. Ann Med Surg (Lond). 2021;68:102554. Figure 2. PMID: 34285804; PMCID: PMC8278239. DOI: 10.1016/j.amsu.2021.102554. License: CC BY 4.0.
Fundus photograph after closed globe injury showing an empty optic disc due to complete optic nerve avulsion, vitreous hemorrhage, and ischemic retinal changes. This corresponds to the optic disc cupping, vitreous hemorrhage, and loss of light perception in complete avulsion discussed in the section “2. Main symptoms and clinical findings.”
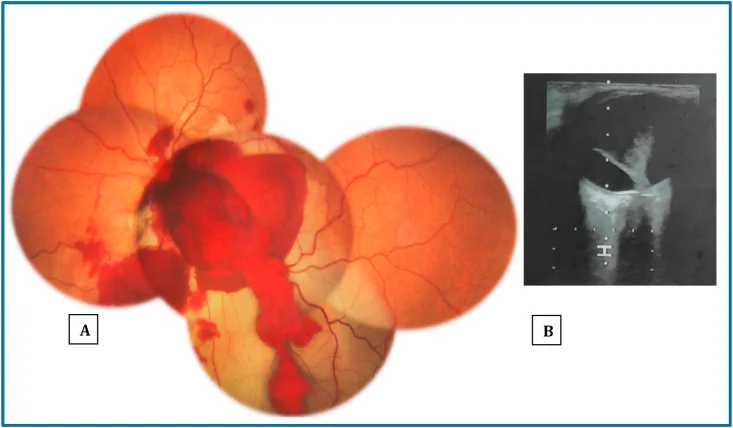
Mahjoub A, Sellem I, Mahjoub A, et al. Optic nerve avulsion: Case report. Ann Med Surg (Lond). 2021;68:102554. Figure 1. PMCID: PMC8278239. License: CC BY.
Initial findings after blunt ocular trauma (fall from horse): (A) Fundus photograph shows extensive vitreous hemorrhage and preretinal hemorrhage covering the optic disc; (B) Ocular ultrasound shows posterior vitreous detachment. This corresponds to the acute fundus and ultrasound findings of optic nerve head avulsion discussed in the section “2. Main symptoms and clinical findings.”
Fundus findings (optic disc): When the media are clear, an abnormally deep optic disc cupping is observed. This is due to a cavity formed by the optic nerve retracting into the dural sheath. Vitreous hemorrhage and peripapillary hemorrhage are frequently associated1).
Normal fundus immediately after injury: The fundus may appear normal immediately after injury. After 6–8 weeks, progressive optic atrophy occurs, and the optic disc becomes pale.
Critical flicker frequency (CFF): Markedly decreased or unmeasurable.
Partial avulsion
Visual acuity: Some visual function may remain.
OCT findings: Deep cavitation of the optic disc is observed. RNFL thinning (reported as 46 μm temporal, 91 μm superotemporal, 60 μm superonasal) 1).
Course: Glial proliferation covers the severed cavity. Glial proliferation becomes prominent after 1 month 1).
Complete Avulsion
Visual acuity: No light perception (NLP).
Fundus: The optic nerve retracts into the dural sheath, forming a deep cavity.
Prognosis: Recovery of visual function is almost impossible. Structural damage is irreversible 4).
As a temporal change in OCT findings, GCC (ganglion cell complex) thickness becomes thinner than normal from 2 weeks after injury. It is known to stabilize around 30–50 days. Fluorescein angiography may show venous branch occlusion and microvascular remodeling 1).
QHow to diagnose when the fundus is not visible due to vitreous hemorrhage?
A
B-mode ultrasonography is useful. It can be detected as a hypoechoic area corresponding to the avulsion site 1). CT and MRI are also used adjunctively. See “Diagnosis and Examination Methods” for details.
Blunt trauma: The most common mechanism 1). A small blunt object or finger enters between the eyeball and the orbital wall. It tends to occur when a strong rotational force is applied, such as when a finger enters the orbit.
Penetrating trauma: Relatively rare but occurs. There is a report of penetrating trauma by a tree branch in an ATV (all-terrain vehicle) accident → eyeball dislocation + optic nerve avulsion 2).
High-risk groups: Males, traffic accident victims, accidental eye injuries during sports, head and facial trauma from falls.
ATV accidents: Open-air high-speed vehicles with no protective equipment, high risk of facial and eye injuries 2).
Rotational external force: Can occur in situations where a strong rotational external force is applied to the face, such as in boxing.
Fundus examination (ophthalmoscopy): Direct diagnosis is possible in cases with clear media. An abnormally deep optic cup is observed. The optic disc is often not visible due to vitreous hemorrhage.
B-mode ultrasound: Useful when the optic disc cannot be observed due to vitreous hemorrhage. Detects hypoechoic areas at the avulsion site 1).
CT scan: First-choice imaging for orbital trauma. Thin-slice CT (0.75–1 mm) is essential; 3 mm slices may miss optic canal fractures or Onodi cell hemorrhage 8). Up to 20% of optic canal fractures may be missed on CT. Scleral wall defects may be identified.
MRI: STIR sequence detects optic nerve swelling and hyperintensity 4). DWI can also detect restricted diffusion of the optic nerve4). In cases of optic nerve avulsion, fluid signal may be seen at the intracanalicular-intracranial junction 4). MRI is contraindicated if metallic foreign bodies are possible.
OCT: Often not useful in the early stage due to media opacity. When media are clear, changes in the ONH and macula can be recorded 1). Useful for tracking GCC thickness changes over time after 2 weeks post-injury.
No effective treatment has been established for optic nerve avulsion. Early diagnosis and avoiding unnecessary treatment are most important. High-dose intravenous steroids have not shown benefit and may cause harm 1). For the irreversible structural change of physical disruption at the lamina cribrosa, no currently available medical intervention can repair the damage. The principle is to avoid unnecessary invasive treatments under appropriate diagnosis and to preserve remaining visual function.
Treatment for Traumatic Optic Neuropathy in General
The following treatments are considered for traumatic optic neuropathy in general, including types other than avulsion.
IONTS (International Optic Nerve Trauma Study): Neither steroid therapy nor optic canal decompression showed clear superiority over observation. Treatment should be individualized 3)7).
Conservative therapy: Early administration of hyperosmotic agents and steroids may be performed.
Optic canal decompression: Visual improvement can be expected when there is an optic canal fracture. It can be performed minimally invasively via endoscopic transnasal approach (ETOND)6). Early surgery (within 24–48 hours of injury) is associated with better prognosis5). If preoperative visual acuity is hand motion or better, the postoperative improvement rate is high5).
Fukumasa et al. (2024) performed optic canal decompression 6 hours after injury in a 10-year-old boy with traumatic optic neuropathy due to optic canal fracture, and administered postoperative prednisolone 25 mg/kg/day. Visual acuity improved from hand motion preoperatively to 20/30 after 12 days, and was maintained at 9 months5). In pediatric traumatic optic neuropathy, visual improvement is reported in approximately 80% of cases.
Tachibana et al. (2024) performed endoscopic optic nerve decompression after methylprednisolone 1 g/day pulse therapy in a 70-year-old man with traumatic optic neuropathy. VA improved from 0.2 to 0.8 (at 6 months)7).
When complicated by submacular hemorrhage: Pneumatic displacement with SF6 gas + intravitreal injection of rtPA 25 μg/0.1 mL may be effective. There is a report of successful displacement of hemorrhage from the submacular area by maintaining prone position for 3 days1).
QIs surgery effective for optic nerve avulsion?
A
There is no established effective treatment for optic nerve avulsion itself. However, in traumatic optic neuropathy with optic canal fracture, optic canal decompression may contribute to visual improvement5). Surgery is not indicated when there is irreversible structural damage such as complete transection4).
The main mechanisms of optic nerve avulsion are classified into indirect and direct injury. Various hypotheses exist regarding the pathogenesis associated with blunt trauma, but in all cases, the unmyelinated nerve fibers of the optic nerve are torn at the structurally vulnerable lamina cribrosa, and then the nerve fibers migrate posteriorly within the nerve sheath.
Vulnerability of the lamina cribrosa: Optic nerve axons lose their myelin sheath and supporting connective tissue at the lamina cribrosa. This site is most susceptible to injury, and most cases occur at the optic disc-globe junction. The core mechanism is that the unmyelinated nerves are torn while the continuity of the optic nerve dura is preserved, and then the nerve fibers migrate posteriorly within the nerve sheath.
Bell’s phenomenon (indirect injury): The defensive reflex that rotates the eye upward and outward during trauma causes rotational distortion of the optic nerve1).
Acute intraocular pressure elevation (indirect injury): A mechanism in which a rapid rise in intraocular pressure due to non-penetrating blunt trauma pushes the optic nerve has been discussed. Cirovic et al.’s computer modeling showed that intraocular pressure can reach up to approximately 300 mmHg1).
Sudden ocular displacement: Shear stress occurs due to rapid forward displacement of the globe or posterior retropulsion of the optic nerve.
Direct injury: Direct damage to the optic disc from penetrating trauma (relatively rare).
Intraorbital transection: Transections further posterior have also been reported. Histopathological findings of absence of neural tissue within the dural sheath have demonstrated continuity disruption within the orbit2).
Glial reaction: In partial transection, the transection cavity becomes covered by glial tissue. Glial proliferation becomes prominent after one month1).
Vascular impairment: Peripapillary vascular changes near the transection site may impair retinal perfusion1). This mechanism also underlies the complication of central retinal artery occlusion.
7. Latest Research and Future Perspectives (Investigational Reports)
LSCI (Laser Speckle Contrast Imaging) is a non-invasive technique for quantitatively assessing optic disc blood flow in traumatic optic neuropathy.
Jallow et al. (2025) detected a decrease in peak BFVi (blood flow velocity index) using LSCI in a 15-year-old male with direct posterior traumatic optic neuropathy: 20.5 a.u. in the healthy eye vs. 13.4 a.u. in the affected eye (at 3 weeks)9). The difference persisted at 6 months (15.1 a.u. vs. 13.7 a.u.). Its potential application in acute trauma assessment is noteworthy.
This is a quantification method using ImageJ macros on Goldmann perimetry, allowing longitudinal tracking of changes in isopter area7). It is applied to evaluate visual field changes in traumatic optic neuropathy.
Experimental approaches such as erythropoietin, brain-derived neurotrophic factor (BDNF), and stem cell therapy are expected to contribute to future optic nerve repair4).
QWhat is LSCI? How might it help diagnose traumatic optic neuropathy?
A
LSCI stands for laser speckle contrast imaging, a non-invasive technique that quantitatively assesses retinal and optic disc blood flow. It has been shown to detect decreased blood flow in eyes with traumatic optic neuropathy compared to healthy eyes9), and its application as an objective evaluation tool in acute trauma is being studied.
Bayram-Suverza M, Rosano-Barragán M, Ramírez-Estudillo J. Long-term follow-up of a patient with partial optic nerve avulsion associated with submacular hemorrhage who underwent pneumatic displacement. Am J Ophthalmol Case Rep. 2024;35. PMCID:PMC11152889.
Omari A, Carniciu AL, Desai M, Schimmel O, Schlachter DM, Folberg R, et al. Globe dislocation and optic nerve avulsion following all-terrain vehicle accidents. American journal of ophthalmology case reports. 2022;27:101621. doi:10.1016/j.ajoc.2022.101621. PMID:35782169; PMCID:PMC9243039.
Tenewitz JE, Chen EJ, Cartwright MJ. A rare presentation of direct traumatic optic neuropathy in a patient poked in the eye by an antenna. Cureus. 2021;13(9):e18244. doi:10.7759/cureus.18244.
Naik SN, Nayak DV. Unravelling the Unseen: A Case Series Exploring the Enigmas of Traumatic Optic Neuropathy. Cureus. 2024;16(12):e75546. doi:10.7759/cureus.75546. PMID:39803156; PMCID:PMC11722660.
Fukumasa H, Yamaga Y, Miyaoka R, Kobayashi M, Nishiyama K. Successful Combination Therapy of Optic Canal Decompression and Steroid Administration for Traumatic Optic Neuropathy in a 10-Year-Old Boy. Cureus. 2024;16(9):e70124. doi:10.7759/cureus.70124. PMID:39449917; PMCID:PMC11501498.
Okui T, Sakamoto T, Morikura I, Okui T, Ayasaka K, Okuma S, et al. Feasibility of navigation-assisted endoscopic transnasal optic nerve decompression for the treatment of traumatic optic neuropathy in patients with midfacial fractures. Journal of the Korean Association of Oral and Maxillofacial Surgeons. 2024;50(5):273-284. doi:10.5125/jkaoms.2024.50.5.273. PMID:39482103; PMCID:PMC11535127.
Tachibana M, Kanno J, Hashimoto M, Hosokawa Y, Sawada M, Nishiyama-Ota Y, et al. Quantification of Goldmann Visual Fields During Resolution of Traumatic Optic Neuropathy. Case reports in ophthalmological medicine. 2024;2024:5560696. doi:10.1155/2024/5560696. PMID:39583778; PMCID:PMC11585370.
Mehta A, Rathod R, Ahuja C, Singh M, Virk RS. Hemorrhage in Onodi Cell Leading to Traumatic Optic Neuropathy. Craniomaxillofacial trauma & reconstruction. 2021;14(1):70-73. doi:10.1177/1943387520922021. PMID:33613839; PMCID:PMC7868511.
Jallow MA, Gholap RS, Asanad S, et al. Laser speckle contrast imaging detects relative blood flow reduction in traumatic optic neuropathy. Am J Ophthalmol Case Rep. 2025;38:102326. doi:10.1016/j.ajoc.2025.102326.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.