The incidence is estimated at 0.15/100,000. 3) It commonly occurs in the 20s to 40s (mean age 25) with no gender predilection. It is often bilateral; even when unilateral at onset, lesions often appear in the fellow eye within days to weeks. 3)
It is a self-limiting disease that resolves spontaneously within 4 to 8 weeks. Visual prognosis is generally good, but some reports indicate visual acuity of 20/25 or worse when the fovea is involved. 7) After resolution, RPE atrophy or pigmentation may remain. Recurrence is rare; if it persists or recurs beyond 6 months, consider transition to Relentless Placoid Chorioretinitis (RPC). 7)
QIs there a risk of blindness from APMPPE?
A
Most cases heal spontaneously, with final visual acuity of 20/25 or better. However, prognosis may be poor if the fovea is involved or if cerebral vasculitis occurs. Rarely, choroidal neovascularization (CNV) may develop and cause vision loss. 11)
Multiple cream-colored to gray-white scaly lesions appear at the level of the posterior pole RPE. Lesion size ranges from 1/4 to 2 disc diameters, with relatively distinct borders.
Active Lesions
Scaly lesions: Multiple cream-colored to gray-white scaly lesions at the posterior pole RPE level, 1–2 disc diameters in size. 11)
Mild vitritis: About 50% of cases have mild vitreous opacities. Anterior uveitis may also be present.
Optic neuritis: 14 cases of optic neuritis have been reported in the literature. 1)
Resolution and Atypical Findings
RPE atrophy and pigment clumping: Lesions resolve within 1–2 weeks, transitioning to RPE atrophy and pigment clumping.
Serous retinal detachment: Rare but reported. Bilateral involvement is considered atypical. 2)
New lesions may appear in the periphery up to 3 weeks after onset. There may be a period where old lesions transition to RPE atrophy and pigment clumping while fresh scaly lesions coexist. Vitreous reaction is usually minimal or absent. 1)Cystoid macular edema (CME) is rare.
Associations with HLA-B7 and HLA-DR2 have been reported. 6) New associations with HLA-B15 and HLA-B35 have also been reported. 5)
QCan APMPPE develop after vaccination?
A
Cases have been reported after various vaccinations, including COVID-19 vaccines. 1)7) It has been suggested that immune activation may trigger choroidal inflammation, but a causal relationship has not been established. If you notice vision changes after vaccination, it is advisable to see an ophthalmologist.
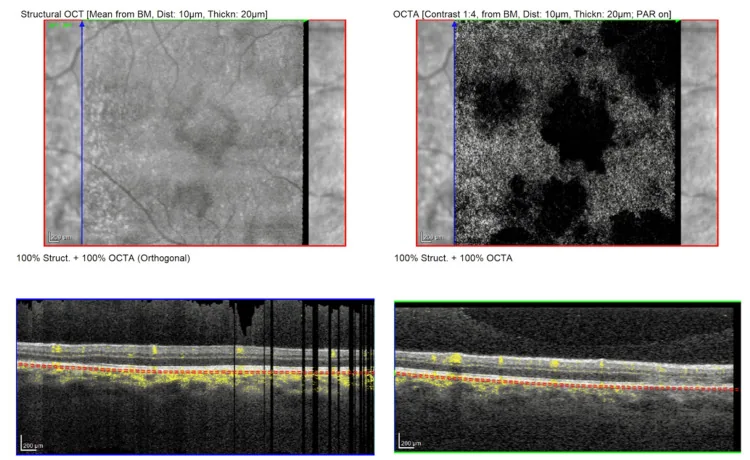
Konstantinos Flindris; Chrysa Chatzipetrou; Eleni Papafotiou; Athanasios Kaliardas; Ioannis Koumpoulis; Ioannis Melissourgos. Unmasking Acute Posterior Multifocal Placoid Pigment Epitheliopathy (APMPPE) Through Multimodal Imaging: A Case Report. Cureus.; 17(6):e86860 Published 2025. Figure 5. PMCID: PMC12296294. License: CC BY.
Optical coherence tomography angiography (OCTA) of the right eye (OD) at presentation, revealing multiple patchy areas of flow reduction (flow voids) at the level of the choriocapillaris corresponding to the placoid lesions
Diagnosis is based on clinical symptoms and fundus findings. Multimodal imaging is useful for understanding the pathology and monitoring the course.
Fluorescein angiography (FA): In the active phase, early hypofluorescence (due to choriocapillaris hypoperfusion or blockage) is seen, which later transforms into irregular hyperfluorescence, a phenomenon known as “fluorescence reversal,” characteristic of APMPPE. 11) In the resolution phase, it remains as a window defect (depigmentation window defect).
Indocyanine green angiography (ICGA): Shows persistent hypofluorescence from early to late phases. This contrasts with FA and reflects impaired perfusion at the choriocapillaris level. 11)
Optical coherence tomography (OCT): In the active phase, hyperreflective lesions extending from the outer plexiform layer to the RPE are observed. Loss of the ellipsoid zone (EZ) suggests foveal involvement and visual decline. 11) Choroidal thickening is also noted. 5) Goldenberg’s OCT classification includes four stages (Stage 1: dome-shaped elevation + EZ disruption, Stage 2: separation of EZ and RPE, Stage 3: RPE hyperreflectivity + EZ/RPE fusion, Stage 4: resolution phase). 2)
Optical coherence tomography angiography (OCTA): Can detect blood flow deficits in the choriocapillaris. 11) Recovery of vascular density with treatment has been reported. 5)
Fundus autofluorescence (FAF): In the active phase, hyperautofluorescence reflecting RPE dysfunction is seen, which transitions to hypoautofluorescence due to RPE cell loss after scar formation. The change from hyper- to hypoautofluorescence is an indicator of scar formation. 8) Hyperautofluorescent lesions in the macula may indicate the need for intensive treatment. 8)FAF is considered superior to ICGA and OCT in differentiating new from old lesions. 8)
Electroretinography (ERG): Shows reduced amplitudes in the active phase, which improve with treatment. 5)
Other differential diagnoses include multiple evanescent white dot syndrome (MEWDS). MEWDS is more common in young women, with white spots distributed extensively to the equator, and shows early hyperfluorescence on FA, differing from APMPPE. Serpiginous choroidopathy is more common in the 40s, is unilateral, and shows progressive enlargement and confluence. 11)
QWhat tests are necessary for the diagnosis of APMPPE?
A
Clinical symptoms and fundus examination are fundamental. FA (reversal phenomenon of fluorescence) is a characteristic finding and useful for diagnosis. Combining multimodal imaging such as OCT, OCTA, FAF, and ICG improves understanding of the pathology and accuracy of follow-up. At initial diagnosis, exclusion of CNS vasculitis by MRI/MRA is also important. 4)
APMPPE is a self-limited disease, and consensus on the indications and methods of treatment has not been established. In cases with good visual acuity and no foveal involvement, observation without treatment is an option. 10)Steroid therapy is recommended for cases with foveal involvement, severe cases, and those complicated by cerebral vasculitis.
Prednisolone: Taper from 0.5 mg/kg/day. Recommended for cases with foveal involvement. Start at 30 mg/day of Predonine tablets (5 mg) and taper over 2 weeks to 1 month.
Methylprednisolone: A protocol of 0.8 mg/kg/day tapered over 7 weeks has been reported. 5)
Steroid pulse therapy
Methylprednisolone infusion: 1,000 mg/day for 3 days of intravenous pulse therapy, followed by a taper of oral prednisolone 60 mg. Used in severe cases and those with cerebral vasculitis. 2)7)
Retrobulbar and sub-Tenon injection: Reports include retrobulbar triamcinolone 20 mg plus dexamethasone 6 mg and sub-Tenon triamcinolone 40 mg. 1)8)
Immunosuppressive therapy
Cases with cerebral vasculitis: Reports of rituximab 375 mg/m² (once weekly for 4 weeks) and mycophenolate mofetil 1,000 mg twice daily. 4)
Long-term immunosuppression: Azathioprine or steroid maintenance for 4 months or longer is recommended for cases with cerebral vasculitis. 6)
Most patients achieve a final visual acuity of 20/25 or better. Many recover within 4 weeks, but up to 6 months of follow-up may be necessary. Foveal involvement is an important predictor of poor prognosis. Permanent scotomas or color vision changes may persist after treatment. 5) There is also a possibility of vision loss due to choroidal neovascularization. 11)
QIs steroid treatment necessary for APMPPE?
A
APMPPE is a self-limiting disease, and no treatment consensus has been established. In cases with good visual acuity and no foveal involvement, spontaneous recovery is common without treatment. 10)Steroid therapy is recommended for cases with foveal involvement or cerebral vasculitis. Treatment decisions should be made on a case-by-case basis.
The most widely supported theory is occlusive vasculitis due to a delayed-type hypersensitivity reaction (type IV allergy) occurring in the afferent arterioles of the choriocapillaris. Primary involvement of the choriocapillaris is thought to occur, with secondary damage to the RPE and outer retina. 11)OCTA has confirmed that outer retinal changes colocalize with blood flow deficits in the choriocapillaris, supporting this hypothesis. 11)
This mechanism is understood as a stepwise pathological process: occlusive vasculitis → choriocapillaris ischemia → hypoperfusion of RPE/photoreceptors. In the past, primary inflammation of the RPE and outer retina was assumed, but it is now considered secondary damage.
As a mechanism for APMPPE onset after COVID-19 infection, it has been proposed that ACE-2 receptors are expressed in the retinal ganglion cell layer, inner plexiform layer, inner nuclear layer, and photoreceptor outer segments, and SARS-CoV-2 RNA has been detected in retinal biopsies of deceased patients. This suggests a pathway of direct infection or molecular mimicry → vascular hyperinflammation → thromboembolism → decreased choroidal perfusion. 9)
EBV may directly infect RPE cells as a reservoir or induce autoimmune inflammation. Involvement of T-lymphocyte activation and type IV hypersensitivity has also been suggested. 10)
Direct Neurotropic Infection Theory (Steptoe Theory)
In some cases, it has been proposed that direct neurotropic infection causes RNFL changes that precede outer retinal changes. However, this is not currently the mainstream theory.
QHas the cause of APMPPE been elucidated?
A
Not confirmed. Occlusive vasculitis of the choriocapillaris is currently the mainstream theory, and the RPE is thought to be secondarily damaged. 11) It is presumed that viral infection or immune activation triggers a delayed-type hypersensitivity reaction (type IV allergy). Research on the mechanism of association with COVID-19 infection and vaccination is also progressing. 9)
7. Latest Research and Future Perspectives (Research Stage Reports)
OCTA can non-invasively quantify blood flow deficits in the choriocapillaris and is becoming the gold standard for diagnosis. 5) It may allow monitoring of changes in vascular density during treatment (at admission vs. 5 weeks later).
Sarna et al. (2025) performed serial evaluations with OCTA and FAF in long-term follow-up cases and reported a correlation between recovery of choriocapillaris blood flow density and improvement in visual function. 5)
Hyperfluorescent lesions on FAF are attracting attention as new indicators of treatment efficacy and risk of scarring. 8)
Yokoi et al. (2022) showed that FAF is superior to ICGA and OCT in distinguishing new and old lesions, and reported its usefulness for treatment monitoring. 8)
New associations with HLA-B15 and HLA-B35 have been reported, and the elucidation of genetic predisposition is progressing. 5) Identification of risk genotypes other than the known HLA-B7 and HLA-DR2 may contribute to prediction of onset and understanding of pathology. 6)
Case reports of APMPPE after COVID-19 infection and mRNA vaccination are increasing, and research is progressing on mechanisms involving molecular mimicry and immune complexes. 2)7)9)
Immunomodulatory therapy for cases with cerebral vasculitis
The efficacy of immunomodulatory drugs such as rituximab and mycophenolate mofetil for severe cerebral vasculitis has been accumulating at the case report level. 4) Further research is needed to establish evidence.
Ogino Y, Namba K, Iwata D, et al. A case of APMPPE-like panuveitis presenting with extensive outer retinal layer impairment following COVID-19 vaccination. BMC Ophthalmol. 2023;23(1):233.