Sarcoidosis is a chronic inflammatory disease of unknown cause characterized by non-caseating granulomas. The lungs, skin, and eyes are commonly affected organs, but when it involves the central nervous system (CNS) and/or peripheral nervous system (PNS), it is called neurosarcoidosis (NS). It may occur alongside sarcoidosis in other organs or affect the nervous system alone.
Incidence: In the United States, it is estimated at 11 per 100,000 white individuals and 35.5–36 per 100,000 African American individuals.
Prevalence: Approximately 152–215 per 100,000 individuals.
Age of onset: 30s–50s. More common in African American women.
Frequency of neurological involvement: Found in 5–15% of sarcoidosis patients4)7). Autopsy evidence in up to 25%, suggesting possible occult involvement.
Neurological onset: In about 70% of cases, neurological symptoms are the initial presentation, often preceding systemic diagnosis3).
In Japan, sarcoidosis is relatively common and is the leading cause of uveitis. It peaks in men in their 20s, and in women shows a bimodal distribution with peaks in their 20s and 50s–60s.
QHow often does neurosarcoidosis occur?
A
Neurological involvement is observed in 5–15% of sarcoidosis patients4)7). Autopsy findings suggest that up to 25% may have neurosarcoidosis, indicating a possible high rate of subclinical cases. In approximately 70% of cases, neurological symptoms are the first sign of the disease3).
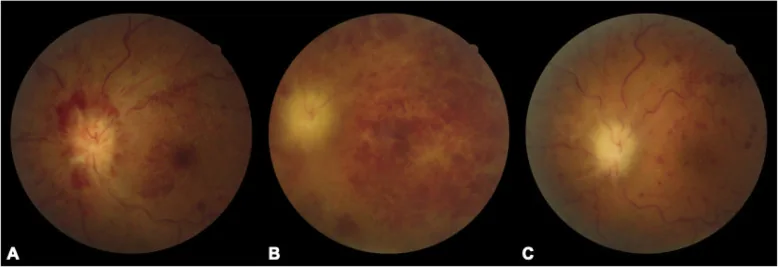
Chaoyi Feng, Qian Chen, Wei Liu et al. Neurosarcoidosis presenting as CRVO combined CRAO: a biopsy-proven case report of a Chinese patient. BMC Ophthalmology. 2020 Aug 27; 20:348. Figure 1. PMCID: PMC7457306. License: CC BY.
Characteristics of optic neuropathy: 28% develop bilaterally in a sequential manner, 37% have optic disc swelling, and 4% have perineuritis10).
QWhat symptoms appear in the eyes?
A
Uveitis is the most common, and granulomatous anterior uveitis with mutton-fat keratic precipitates and iris nodules is characteristic. Ocular sarcoidosis is suspected when two or more of the six IWOS criteria (granulomatous anterior uveitis, angle nodules, snowball vitreous opacities, retinal perivasculitis, candlewax retinal exudates, and optic nerve head/choroidal granuloma) are present. In optic neuropathy, 28% of cases are bilateral 10).
The etiology of NS remains unknown. The basic pathology is non-caseating granuloma formation due to Th1 cell-mediated immune response (type IV allergy). It is hypothesized that prolonged exposure to antigenic stimuli leads to excessive activation of macrophages and T cells. In Japan, there are reports suggesting the involvement of Propionibacterium acnes.
The diagnosis of NS is made by integrating diverse clinical findings and test results. Although definitive diagnosis requires histological confirmation of non-caseating granulomas, CNS biopsy carries risks, so multiple diagnostic criteria are used.
Serum ACE: Elevation is useful for diagnostic support (e.g., 73 U/L9)). Useful for systemic sarcoidosis but specificity for neurosarcoidosis is insufficient
Serum lysozyme: Elevated
Serum soluble IL-2R (sIL-2R): Elevated. Along with lymphopenia, it is a useful marker for ocular sarcoidosis
67Ga-citrate scintigraphy or FDG-PET: Positive uptake aids diagnosis
Gadolinium-enhanced MRI: Most sensitive. Diffuse/thick leptomeningeal enhancement is the most common finding. The combination of periventricular distribution and leptomeningeal enhancement is typical1)
Chest CT: Confirms BHL. In Caucasians, sarcoidosis cannot be ruled out even if chest CT is normal
FDG-PET: Useful for evaluating lesions in other sites and selecting biopsy sites3)
MRI vessel wall imaging (VWI): Useful for evaluating vasculitis-related NS
Confirmation of non-caseating granulomas is the gold standard. CNS biopsy is ideal but highly invasive, so alternative sites such as lymph nodes, skin, conjunctiva, and transbronchial lung biopsy are considered.
QWhat tests are necessary for a definitive diagnosis of neurosarcoidosis?
A
Definitive diagnosis requires histological confirmation of non-caseating granulomas via CNS biopsy. However, due to its invasiveness, a stepwise diagnostic approach combining cerebrospinal fluid analysis (elevated protein, lymphocytosis), gadolinium-enhanced MRI, serum ACE and sIL-2R, and chest CT (to confirm BHL) is often used in practice. If non-caseating granulomas are confirmed in other sites (e.g., lymph nodes, skin, transbronchial lung biopsy), a probable diagnosis can be made.
Because this disease fluctuates in severity, mild cases may be observed with only steroid eye drops, expecting spontaneous remission. Severe cases require systemic steroid administration.
Anterior Uveitis
Steroid eye drops: Rinderon 0.1% 4 times daily. Even in the absence of anterior chamber inflammation, continue to prevent angle nodules.
Mydriatic agents: Mydrin P 3 times daily (to prevent posterior synechiae)
Posterior segment inflammation (severe cases)
Oral steroids: Prednisolone 0.5–1.0 mg/kg/day, starting dose then tapered
An example of a prednisolone tapering regimen is shown below.
Duration
Dose
2 weeks
30 mg/day
1 month
20 mg/day
1 month
15 mg/day
1 month
10 mg/day
1 month
7.5 mg/day
1 month
5 mg/day
1 month
5 mg every other day
Posterior sub-Tenon injection: Sustained-release steroid (Kenacort A 40 mg). Effective for cystoid macular edema and vitreous opacity. Peak effect at about 1 month, duration about 3 months.
Treatment of ocular complications
Complicated cataract: Surgery during the quiescent phase. Can be performed under oral steroid therapy.
Oral corticosteroids: First-line for mild to moderate cases.
Intravenous corticosteroids (pulse therapy): For severe or steroid-resistant cases. Methylprednisolone 1 g for 5 days, followed by oral prednisolone 1 mg/kg6).
Second-line
Methotrexate (MTX): The most frequently used immunosuppressant. It takes time to take effect, so it is used in combination with steroids.
Infliximab: TNF-α inhibitor. Also used in cases with cerebral vasculitis.
Adalimumab: Also a TNF-α inhibitor. Increasingly used in refractory cases.
Cases with cerebral vasculitis: The combination of glucocorticoid + MTX/cyclophosphamide/infliximab is a major treatment strategy7). The hazard ratio for cerebrovascular events within 5 years after sarcoidosis diagnosis is markedly high at 10.067).
Epilepsy complication: Antiepileptic drugs such as levetiracetam are used concomitantly5).
Hormone replacement with hydrocortisone, levothyroxine, and desmopressin (for diabetes insipidus) is necessary for panhypopituitarism due to pituitary lesions. Nerve damage is often irreversible and may require lifelong replacement 4).
QHow long does steroid treatment last?
A
The treatment varies greatly depending on disease severity. In ocular sarcoidosis, prednisolone is typically tapered from 30 mg to 5 mg every other day over approximately 7 months. In severe or recurrent cases, a maintenance dose (5–10 mg/day) may be required long-term. Neurosarcoidosis often relapses and remits, making long-term follow-up essential.
Th1 cells release IL-2 and IFN-γ, recruiting and activating macrophages. Activated macrophages secrete cytokines, sustaining continuous granuloma formation. Histologically, epithelioid cells and multinucleated giant cells form the center, surrounded by lymphocytes, plasma cells, and mast cells. Asteroid bodies may be observed within multinucleated giant cells.
Granulomas form within or around the vessel wall, particularly in small penetrating arteries. The hazard ratio for cerebrovascular events within 5 years after sarcoidosis diagnosis is 10.06, indicating a markedly elevated risk of cerebrovascular complications 7).
CSF flow obstruction due to granulomatous scarring of the meninges and impaired CSF absorption due to inflammation of the arachnoid villi occur. Both communicating and non-communicating types can occur2).
Granulomatous infiltration of the hypothalamus, pituitary stalk, and pituitary gland disrupts the endocrine axis. In severe cases, central diabetes insipidus with Na 168 (hypernatremia) may be present4).
7. Latest Research and Future Prospects (Research-Stage Reports)
MRI vessel wall imaging technology is expected to improve the diagnostic accuracy of vasculitis-related NS.
In a systematic review by Focke et al. (2025), MRI VWI successfully detected vessel wall lesions in 9 of 13 NS patients (69%)7). This technique may visualize vessel wall inflammation that is difficult to detect with conventional gadolinium-enhanced MRI.
Neopterin and lysozyme in CSF are attracting attention as biomarkers for vasculitis-associated neurosarcoidosis.
Focke et al. (2025) reported that CSF neopterin was elevated in 100% of cases (mean 5.2 ng/ml) and lysozyme in 75% (mean 4.25 mg/l) in patients with vasculitis-associated neurosarcoidosis7). These markers may serve as diagnostic tools.
As imaging alternatives to FDG-PET, somatostatin receptor imaging and PET imaging targeting CXCR4 (expressed on activated macrophages) are being explored.
Ach T, Ben Yahia W, Halloul I, Sghaier F, Atig A. Neurosarcoidosis-Induced Hypophysitis Mimicking Pituitary Macroadenoma. Cureus. 2023;15(6):e39865. doi:10.7759/cureus.39865. PMID:37404438; PMCID:PMC10315063.
Kafai Golahmadi A, Craven CL, Watkins LD. Neurosarcoidosis Mimicking Normal Pressure Hydrocephalus. Cureus. 2023;15(6):e40281. doi:10.7759/cureus.40281. PMID:37448383; PMCID:PMC10336621.
Hanif Z, Gonzalez Ramos KN, Razminia P, Aigbe E, Ghafourian P. A Perplexing Case of Bladder Mass Biopsy-Proven Neurosarcoidosis. Cureus. 2023;15(6):e40865. doi:10.7759/cureus.40865. PMID:37489187; PMCID:PMC10363404.
Khawaja MA, Awesat BE, Yasini MN, et al. Neurosarcoidosis Presented as an Isolated Brain Lesion. Cureus. 2023;15(9):e45837. doi:10.7759/cureus.45837.
Chaubey M, Meena K, Singh T, Reddy S, Raj R, Chaudhary A, et al. Neurosarcoidosis: An under-diagnosed cause of myelopathy. Journal of family medicine and primary care. 2024;13(5):2157-2160. doi:10.4103/jfmpc.jfmpc_987_23. PMID:38948561; PMCID:PMC11213433.
Focke JK, Brokbals M, Becker J, Veltkamp R, van de Beek D, Brouwer MC, et al. Cerebral vasculitis related to neurosarcoidosis: a case series and systematic literature review. Journal of neurology. 2025;272(2):135. doi:10.1007/s00415-024-12868-2. PMID:39812656; PMCID:PMC11735521.
Ryan Shields, Olivia Sagan, Logan Roebke, Josh Vander Maten, Shailen Shah, George Chang, Dalia Ibrahim, Sumayya Naz. Rare case of multifocal extradural and intramedullary neurosarcoidosis without pulmonary involvement: a case report and literature review. Spinal Cord Ser Cases. 2021;7(1). doi:10.1038/s41394-021-00450-1.
Sarac E, Erzurum SA, Arif A. An Unusual Presentation of Neurosarcoidosis. Am J Case Rep. 2022;23:e937125. doi:10.12659/ajcr.937125.
Desmond PK, Ben JB, Elizabeth MG, Gordon TP. Optic neuropathy associated with systemic sarcoidosis. Neurol Neuroimmunol Neuroinflammation. 2016;3:e270.
Kidd D, Beynon HL.. The neurological complications of systemic sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis. 2003;20(2):85-94. PMID:12870717.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.