Neuro-ophthalmic signs of COVID-19 refer to a variety of clinical manifestations resulting from damage to the neuro-ophthalmic system, including the optic nerve, cranial nerves, visual pathways, and pupillary pathways, associated with SARS-CoV-2 infection (COVID-19).
SARS-CoV-2 was first reported in Wuhan, China in 2019, and the WHO declared a pandemic in March 2020. It has since spread to over 223 countries, causing more than 770 million confirmed cases and approximately 7 million deaths (WHO). In 2020, it became the third leading cause of death in the United States after heart disease and cancer. Neurological complications have been reported in about 4% of severe COVID-19 patients 1), with the highest risk of severe illness in individuals aged 60 and older with underlying medical conditions.
QHow common are neuro-ophthalmic symptoms in COVID-19?
A
Neurological complications have been reported in about 4% of severe COVID-19 cases 1). Headache occurs in up to 71% of SARS-CoV-2-positive individuals, and eye pain in 34%. Neuro-ophthalmic signs such as optic neuritis and cranial nerve palsy may appear during or after infection.
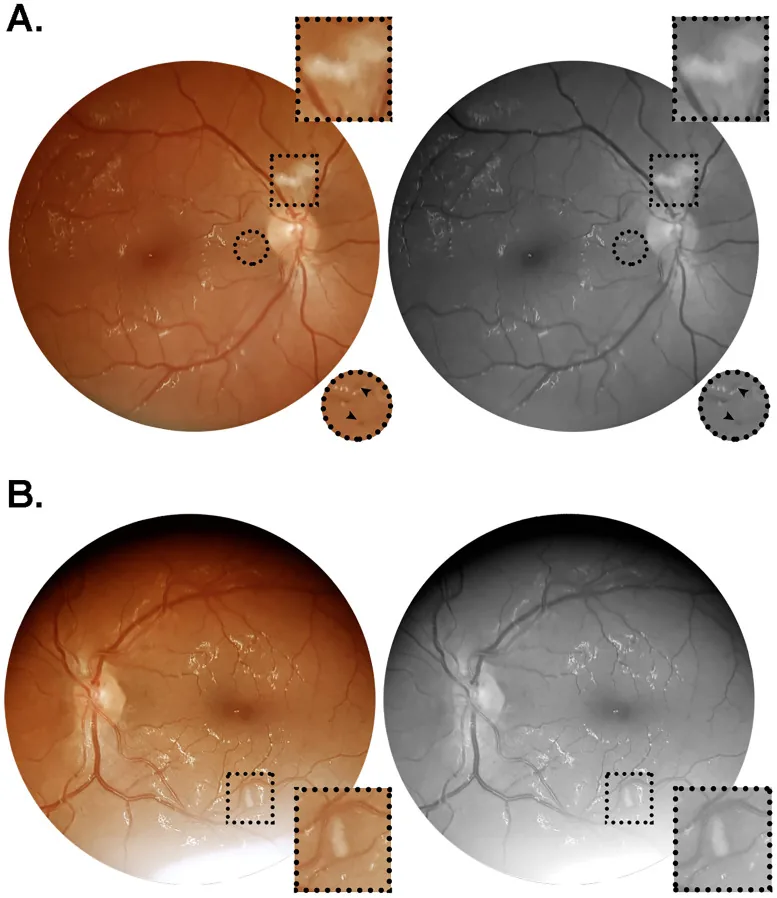
Rafael Lani-Louzada, Carolina do Val Ferreira Ramos, Ricardo Mello Cordeiro et al. Retinal changes in COVID-19 hospitalized cases. PLoS ONE. 2020 Dec 3; 15(12):e0243346. Figure 1. PMCID: PMC7714146. License: CC BY.
Illustration showing the main symptoms of COVID-19 eye infection
Optic disc phlebitis: Decreased visual field sensitivity, retinal vascular dilation and tortuosity, papilledema, retinal hemorrhage.
Optic neuroretinitis: Acute unilateral vision loss, optic disc swelling, and perifoveal star-shaped hard exudates.
Cranial Nerves and Ocular Motor System
Cranial nerve palsy: Single or multiple involvement of cranial nerves III, IV, VI, and VII. Occurs in the context of Fisher syndrome, Guillain-Barré syndrome, and myasthenia gravis.
Nystagmus and ocular motor disorders: Associated with BPPV, acute labyrinthitis, rhombencephalitis, and Bickerstaff brainstem encephalitis. Opsoclonus-myoclonus-ataxia syndrome (OMAS) has also been reported.
Pupillary abnormalities: Adie tonic pupil (days to 1 month after infection), Horner syndrome (associated with pneumonia affecting the upper lung).
Idiopathic intracranial hypertension (IIH): Frequently reported in children due to MIS-C.
Secondary infection (ROCM): Rhino-orbital-cerebral mucormycosis. 87% have a history of steroid use, 78% have diabetes.
QWhat causes double vision after COVID-19?
A
Double vision after COVID-19 is mainly caused by cranial nerve III, IV, and VI palsy. It can also occur in the context of Fisher syndrome (characterized by the triad of ophthalmoplegia, ataxia, and areflexia), Guillain-Barré syndrome, and myasthenia gravis. Cases associated with cerebral venous sinus thrombosis (CVST) have also been reported.
SARS-CoV-2 is an enveloped, positive-sense single-stranded RNA virus belonging to the family Coronaviridae. The spike (S) protein binds to the ACE2 receptor to enter host cells. ACE2 receptors are expressed not only in respiratory epithelium but also in neurons and glial cells of the brain.
The following routes of entry into neural tissue have been proposed:
Olfactory nerve route: Direct central nervous system invasion via the olfactory nerve.
Meningeal/choroid plexus route: Entry bypassing the blood-brain barrier.
Hematogenous route: Invasion via systemic circulation due to viremia.
Direct neuronal damage: Direct invasion of nerve cells by the virus.
Cytokine storm: Immune activation of monocytes, neutrophils, and T lymphocytes triggers local and systemic inflammation, increasing vascular permeability.
Abnormal autoantibody production: Immune-mediated nerve damage, such as positivity for anti-MOG antibodies.
SARS-CoV-2 infection has been reported as a risk factor for non-arteritic anterior ischemic optic neuropathy (NA-AION). 2) The proposed mechanism is inflammatory/autoimmune thrombotic microangiopathy. NA-AION has also been reported after COVID-19 vaccination. 2)
QCan neuro-ophthalmic complications occur after COVID-19 vaccination?
A
After vaccination, optic neuritis, bilateral AION, cerebral venous thrombosis, pupillary abnormalities (Horner syndrome, Holmes-Adie pupil), acute ischemic stroke, BPPV, and others have been reported. Acute macular neuroretinopathy (AMN) has also been suggested to be directly associated with vaccination or infection.
Visual field test: Central/paracentral scotoma is typical in optic neuritis, while altitudinal hemianopia is typical in anterior ischemic optic neuropathy (AION).
Visual evoked potential (VEP): In demyelinating diseases, it shows prolonged latency; in ischemic diseases, only reduced amplitude.
Orbital MRI: Useful for identifying abnormal enhancement associated with optic neuritis. Coronal fat-suppressed STIR and contrast-enhanced T1-weighted images are particularly useful.
FLAIR images: Used to evaluate demyelinating lesions (assessment of MS comorbidity).
DWI (diffusion-weighted imaging): Useful for evaluating stroke and optic nerve ischemia.
In the differential diagnosis of optic neuritis, ischemic, compressive, neoplastic, sinus-related, toxic, and hereditary optic neuropathies must be excluded. Features of atypical optic neuritis include the following.
Onset outside the age range of 15 to 45 years
Bilateral onset
Progression after 2 weeks from onset
Steroid dependence
Systemic symptoms
Evaluation of anti-AQP4 and anti-MOG antibodies is also important for differential diagnosis. For differentiation from NA-AION, refer to age, presence of pain, visual field pattern, and VEP findings. 2)
Systemic management of COVID-19 includes anti-SARS-CoV-2 monoclonal antibodies, antiviral drugs, immunomodulators, and corticosteroids. For respiratory failure, monitoring with pulse oximetry and maintaining oxygen saturation at 92–96% is fundamental.
Dexamethasone or remdesivir has been reported to be associated with a reduced frequency of neurological complications including stroke, seizures, and meningitis. Combination of both drugs shows a synergistic effect, and dexamethasone also reduced the risk of neurological complications in non-hypoxic COVID-19. 1)
Arteritic AION (GCA-related): High-dose intravenous corticosteroids 1 g/day for 3–5 days, followed by oral prednisolone 1 mg/kg/day tapered over 4–6 months.
Non-arteritic AION (NA-AION): Currently, there is no treatment with clear efficacy for improving visual function in the acute phase or preventing onset in the fellow eye.
Management is based on addressing inflammation, ischemia, hypercoagulable states, and systemic abnormalities (hypertension, hypoxia). For stroke-related cases, therapeutic anticoagulation, intravenous thrombolysis, and mechanical thrombectomy are options. Immunosuppressive drugs should be used with caution in active infections due to the risk of infectious complications. Currently, there are no standard screening protocols or established decision-making algorithms.
QHow is optic neuritis associated with COVID-19 treated?
A
The basic treatment for optic neuritis is steroid pulse therapy (methylprednisolone 1,000 mg/day intravenously for 3 days). This treatment is mandatory for atypical optic neuritis (bilateral, steroid-dependent, systemic complications, etc.). If NMO spectrum disorder or collagen disease is suspected, collaboration with a neurologist is necessary.
The spike (S) protein of SARS-CoV-2 binds to the ACE2 receptor to enter host cells. ACE2 receptors are widely distributed in respiratory epithelium, esophagus, cardiomyocytes, bladder urothelium, renal proximal tubules, and the brain (neurons and glial cells).
The following pathways are thought to be involved in the pathogenesis of neuro-ophthalmic signs.
Direct neural damage: The virus invades the central nervous system via the olfactory nerve, meninges, choroid plexus, or hematogenous route, directly damaging neurons and glial cells.
Cytokine storm: Activation of monocytes, neutrophils, and T lymphocytes triggers local and systemic inflammation, leading to increased vascular permeability and pulmonary edema. This systemic inflammation contributes to secondary damage to neural tissue.
Immune-mediated mechanisms: Abnormal autoantibody production (e.g., anti-MOG antibodies) is induced, causing optic neuritis and neuromyelitis optica spectrum disorders.
Hypercoagulable state: Persistent pro-inflammatory conditions increase the risk of cerebral venous sinus thrombosis (CVST) and stroke.
Neuro-ophthalmologic signs appear simultaneously with systemic symptoms or within a few days to weeks.
The presumed mechanism of NA-AION is inflammatory/autoimmune thrombotic microangiopathy due to SARS-CoV-2 infection. 2)In vaccine-related neuro-ophthalmologic complications, acute macular neuroretinopathy (AMN) due to microvascular ischemia of the choriocapillaris has been reported.
Neuro-ophthalmologic symptoms in long COVID are presumed to be maintained by chronic inflammation and persistently increased cytokine production.
7. Latest Research and Future Prospects (Investigational Reports)
Grundmann et al. (2022) reported in an analysis of patients with severe COVID-19 that treatment with dexamethasone or remdesivir was associated with a reduced frequency of neurological complications including stroke, seizures, and meningitis 1). Combination of both drugs showed a synergistic effect, and dexamethasone also reduced the risk of neurological complications in non-hypoxic COVID-19. Further investigation is needed to determine the role of these drugs in preventing neurological complications.
Associations between both COVID-19 infection and vaccination with giant cell arteritis (GCA) have been reported, and further accumulation of evidence is expected.