Cerebral venous and dural sinus thrombosis (CVST) is a thrombus in the cerebral venous drainage system and a rare type of stroke. Some patients present to ophthalmology with papilledema and visual disturbances due to increased intracranial pressure (ICP).
Historical background: In 1825, Ribes MF reported the first case in a 45-year-old man (headache, seizures, delirium; autopsy confirmed superior sagittal sinus and transverse sinus thrombosis). In 1828, Abercrombie reported the first puerperal CVST (a 25-year-old woman 2 weeks after uncomplicated delivery, with headache and seizures).
Epidemiology is as follows:
Incidence: 0.5–3% of all strokes, 0.5–1.0% of all cerebrovascular diseases3)
Annual incidence: approximately 5 per million people (up to 15.7 per million reported2))
Age and sex: More common in young people under 50 years old, and more common in women (due to hormone-specific risk factors)
Major studies: Italian multicenter study (706 patients), International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVDST, 624 patients)
Notably, COVID-19-associated CVST has different demographic characteristics from conventional CVST, with 56% male and a mean age of 51.8±18.2 years2).
QHow rare is CVST?
A
It accounts for 0.5–3% of all strokes, with an incidence of about 5 per 100,000 person-years, and is classified as a rare disease. However, recognition has improved with advances in neuroimaging, and special attention is needed in young women and pregnant/postpartum women.
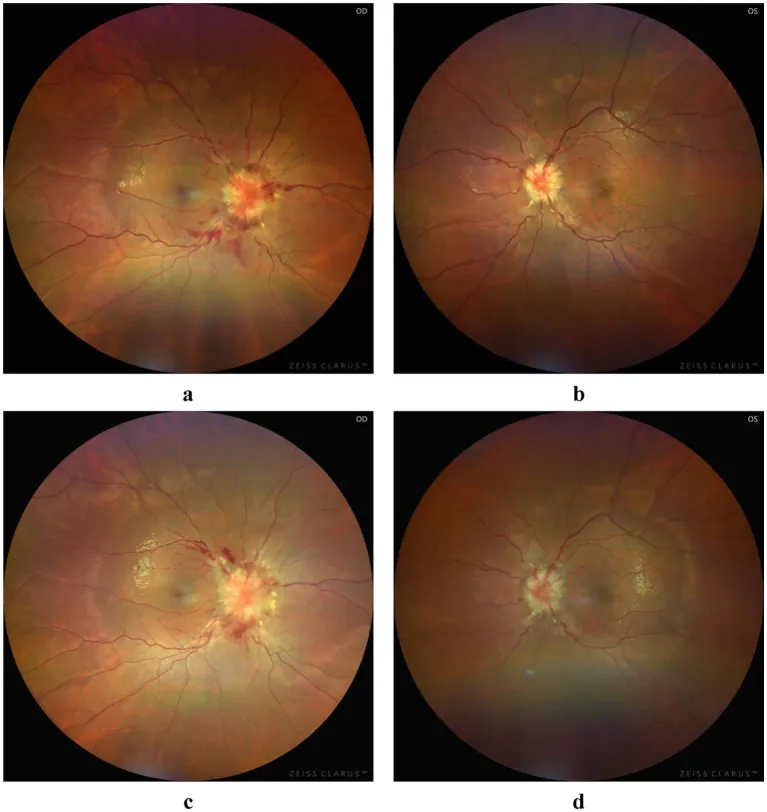
Ligang Jiang et al. Atypical bilateral papilledema during the puerperium: a case report. Frontiers in Medicine. 2025 Jul 4; 12:1636933. Figure 1. PMCID: PMC12271223. License: CC BY.
Papilledema: Present in 28.3% of ISCVST. Directly related to increased ICP. Ophthalmoscopic findings include bilateral optic disc redness and swelling, blurred disc margins, and retinal vein dilation. Fluorescein angiography shows dye leakage from the disc. Optical coherence tomography (OCT) detects abnormal nerve fiber layer thickness. Note that in eyes with optic atrophy from prior papilledema, increased ICP cannot be ruled out even without papilledema.
Homonymous hemianopsia: Occurs with venous infarction of the occipital lobe.
Venous pulsations: Present in 90% of normal individuals. If venous pulsations are observed, increased intracranial pressure can be ruled out.
QWhat is the most common symptom of CVST?
A
Headache is the most common symptom (88.8% in ISCVST) and may be the only presenting symptom. Visual disturbances occur in 13.2% and diplopia in 13.5%, which may prompt an ophthalmology visit. Headache alone is particularly easy to miss; fundus examination should be actively performed in patients suspected of increased ICP.
The etiology of CVST involves various risk factors related to Virchow’s triad (stasis of blood flow, changes in blood composition, and vessel wall abnormalities). Approximately 12.5% are idiopathic with unknown cause.
Hormonal Factors
Pregnancy and postpartum period: The third trimester and the first month after delivery are particularly high risk. The mortality rate of pregnancy-related CVST is 5–30%3).
Oral contraceptives: A major risk factor more common in women.
Hormone replacement therapy: Increased coagulation due to estrogen preparations.
Thrombophilia
Inherited thrombophilia: Factor V Leiden mutation, antithrombin III deficiency, protein C/S deficiency.
Antiphospholipid syndrome: Positive for antiphospholipid antibodies and anticardiolipin antibodies.
Infections: Parameningeal infections, COVID-19 infection. CNS infections account for 2.1% of all CVST cases but are a poor prognostic factor3).
Inflammatory bowel disease: The overall VTE risk in IBD patients is about 3.4 times higher, and 8.4 times during flares (cohort of 13,756 cases)5). The estimated incidence of CVST in IBD is 1.3–6.4%5).
Specific medications: Androgens, danazol, lithium, vitamin A, IVIG, infliximab.
Others: Obesity, low intracranial pressure, high altitude, hypercoagulable state in cancer.
Pediatric CVST: L-asparaginase and corticosteroids used in chemotherapy for acute lymphoblastic leukemia (ALL) increase the risk of thrombosis 4). Obesity is also an independent risk factor in children 4).
COVID-19-associated CVST: Venous thromboembolism (VTE) occurs in 22.7% of ICU patients and 7.9% of non-ICU patients, with reported incidence of COVID-19-associated CVST at 0.3–0.5% 2). The average time from COVID-19 onset to CVST diagnosis is 15.6 ± 23.7 days 2), and the risk of CVST persists for 2 weeks after infection.
QIs there a risk of developing CVST after COVID-19 infection?
A
The incidence of COVID-19-associated CVST is 0.3–0.5%, with an average time to onset of 15.6 days (wide range) after COVID-19 onset 2). If headache, visual symptoms, or seizures occur after COVID-19 infection, evaluation for CVST should be considered.
MRI/MRV: The most sensitive test for identifying CVST. MRV is optimal for pregnant women (non-invasive, no radiation) 3). MRI signal changes depend on the age of the thrombus (see table below).
CT/CTV: Non-contrast head CT has low specificity for CVST, showing abnormalities in only about 30% of cases. CTV is added when MRI/MRV is unavailable. The empty delta sign (a high-density triangle in the posterior superior sagittal sinus) is a characteristic finding.
Suspected IIH (with papilledema): Both MRI and MRV are recommended.
The characteristic MRI signal changes by stage are shown below.
The main differential diagnoses are idiopathic intracranial hypertension (IIH), intracranial tumor, brain abscess, intracerebral hemorrhage, ischemic stroke, meningoencephalitis, autoimmune encephalitis, paraneoplastic encephalitis, and neuromyelitis optica. Consider IIH when CVST is ruled out in patients with papilledema.
Close monitoring of visual acuity and visual field is important in patients with ICP elevation. If ICP is reduced early, papilledema resolves quickly and visual function recovers without impairment. If treatment is delayed and visual impairment occurs, it becomes irreversible.
QCan anticoagulation therapy be performed even if there is intracranial hemorrhage associated with CVST?
A
Intracranial hemorrhage associated with CVST is not an absolute contraindication to heparin therapy. Anticoagulation therapy may be considered beneficial from the perspective of improving venous outflow obstruction and preventing worsening of hemorrhage. However, judgment by a specialist based on individual conditions is essential.
QWhat is the visual prognosis of CVST?
A
Complete recovery is achieved in 79% of all cases. Visual prognosis depends on the promptness of optic nerve decompression; early reduction of ICP leads to rapid resolution of papilledema and preservation of visual function. On the other hand, if visual dysfunction appears due to treatment delay, it becomes irreversible. If papilledema does not improve with vascular treatment, ONSF should be considered.
In CVST, thrombi most commonly form at the confluence of cerebral veins and large venous sinuses. The dural venous sinuses contain arachnoid granulations (structures that drain CSF from the subarachnoid space into the systemic venous system), and thrombus formation impedes CSF drainage, leading to increased ICP.
The pathogenetic cascade is as follows.
Cortical vein occlusion → increased hydrostatic pressure in veins and capillaries → disruption of the blood-brain barrier (BBB) → vasogenic edema → sustained increase in ICP → rupture and hemorrhage of veins and capillaries, decreased cerebral perfusion → ischemia and cytotoxic edema
Because the cortical venous system is anatomically variable, clinical findings depend on the size, extent, location of the thrombus, and the state of collateral circulation. In many cases, dural sinus thrombosis and cortical vein thrombosis occur simultaneously.
Four Pathophysiological Mechanisms of Visual Impairment
Arachnoid granulation impairment: CSF retention → stagnation of axonal flow → papilledema. It may be difficult to differentiate from idiopathic intracranial hypertension (IIH).
Venous Infarction Type
Infarction of the geniculo-calcarine pathway: especially venous infarction of the primary visual cortex → homonymous hemianopia. It results from impaired venous drainage of the occipital lobe.
Dural arteriovenous fistula type
Secondary dural arteriovenous fistula: Develops as a late complication of CVST. Increased ICP due to arteriovenous fistula causes visual impairment.
Brain herniation type
Brain herniation due to massive venous infarction: Mass effect → occipital lobe arterial infarction → ischemic damage to the visual cortex. This is the most severe mechanism.
Mechanism of papilledema: Increased pressure in the subarachnoid space around the optic nerve compresses the optic nerve, leading to stagnation of axoplasmic flow and formation of optic disc edema.
In a systematic review of 43 cases by Panichpisal et al. (2022), D-dimer, fibrinogen, and fibrin degradation products were significantly elevated in COVID-19-associated CVST compared to healthy controls 2). Endothelial injury due to interaction of SARS-CoV-2 with ACE receptors and cytokine storm prominent in the second week of infection are thought to increase VTE risk.
Tatsuoka et al. (2021) reported a case of a 28-year-old female Crohn’s disease patient who developed CVST 5 days after the 22nd cycle of high-dose infliximab (IFX) (10 mg/kg) 5). It is thought that a decrease in serum TNF-α due to IFX (anti-TNF-α antibody) administration leads to compensatory upregulation of TNF-α receptors, resulting in “paradoxical thrombus formation.” Cytokine release due to infusion reaction → platelet aggregation → DIC-like thrombus formation is also proposed as a mechanism. The patient fully recovered after emergency decompressive craniectomy and LMWH.
7. Latest research and future perspectives (reports under investigation)
Outcomes of COVID-19-associated CVST have been clarified by large-scale reviews as follows.
In a review of 43 cases by Panichpisal et al. (2022), the mortality rate of COVID-19-associated CVST was 39%, similar to pre-pandemic CVST (4%) and COVID-19-associated mortality of arterial ischemic stroke (38%) 2). Involvement of the deep cerebral venous system was significantly associated with poor prognosis (superficial venous system was associated with good outcome), and good outcome (mRS ≤ 2) was only 52%. 44% of COVID-19-associated CVST had pre-existing thrombotic risk factors, suggesting that COVID-19 may unmask pre-existing predispositions.
Updates to clinical guidelines: The AHA 2024 “Diagnosis and Management of Cerebral Venous Thrombosis: a Scientific Statement” (Saposnik et al., Stroke 2024; 55:e77-90) has been published, and the latest diagnostic and management guidelines are being developed.
Difficulty in predicting IFX-related thrombosis: It has been reported that the onset of thrombosis after IFX administration ranges from the 1st to the 33rd dose, and from 30 minutes to 4 weeks after administration 5), and it is increasingly recognized as a complication that is difficult to predict with standard risk assessment.
Dakay K, Cooper J, Bloomfield J, Overby P, Mayer SA, Nuoman R, et al. Cerebral Venous Sinus Thrombosis in COVID-19 Infection: A Case Series and Review of The Literature. Journal of stroke and cerebrovascular diseases : the official journal of National Stroke Association. 2021;30(1):105434. doi:10.1016/j.jstrokecerebrovasdis.2020.105434. PMID:33190109; PMCID:PMC7833244.
Panichpisal K, Ruff I, Singh M, et al. Cerebral venous sinus thrombosis associated with coronavirus disease 2019: case report and review of the literature. Neurologist. 2022;27(5):253-262.
He J, He Y, Qin Y, Liu L, Xu M, Liu Q. Pregnancy-related intracranial venous sinus thrombosis secondary to cryptococcal meningoencephalitis: a case report and literature review. BMC infectious diseases. 2024;24(1):1155. doi:10.1186/s12879-024-10054-3. PMID:39402460; PMCID:PMC11476198.
Liu J, Yang C, Zhang Z, Li Y. Cerebral venous sinus thrombosis in a young child with acute lymphoblastic leukemia: a case report and literature review. J Int Med Res. 2021;49(1):300060520986291. doi:10.1177/0300060520986291.
Tatsuoka J, Igarashi T, Kajimoto R, Kobayashi M, Moro N, Suma T, et al. High-dose-infliximab-associated Cerebral Venous Sinus Thrombosis: A Case Report and Review of the Literature. Internal medicine (Tokyo, Japan). 2021;60(16):2677-2681. doi:10.2169/internalmedicine.6447-20. PMID:33678739; PMCID:PMC8429287.
Wang Z, Xia H, Fan F, et al. Survival of community-acquired Bacillus cereus sepsis with venous sinus thrombosis in an immunocompetent adult man: a case report and literature review. BMC Infect Dis. 2023;23(1):213. doi:10.1186/s12879-023-08176-1.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.