1. What isPapilledema refers to swelling of the optic disc secondary to elevated intracranial pressure (ICP). This term is used exclusively for disc swelling due to elevated ICP; swelling from other causes is called optic disc edema. In Japan, it is also referred to as “choked disc”.ic dPapilledema refers to swelling of the optic disc secondary to elevated intracranial pressure (ICP). This term is used exclusively for disc swelling due to elevated ICP; swelling from other causes is called optic disc edema. In Japan, it is also referred to as “choked disc”.s also important.
Epidemiology: The annual incidence of idiopathic intracranial hypertension in the United States is 1.15 per 100,000 people 2), with a higher rate in women (1.97 vs 0.36 per 100,000 in men). The highest incidence is in the reproductive age group of 18–44 years (2.47 per 100,000), and it is increasing worldwide with the obesity epidemic 2). Normal adult ICP measured by manometer is less than 250 mmH2O, and in children less than 280 mmH2O.
QWhat is the difference between papilledema and optic disc edema?
A
Papilledema is a term limited to elevated ICP, while disc swelling from other causes (e.g., optic neuritis, ischemia, infiltrative lesions) is called optic disc edema. This distinction is important because it directly guides identification of the etiology and selection of appropriate treatment.
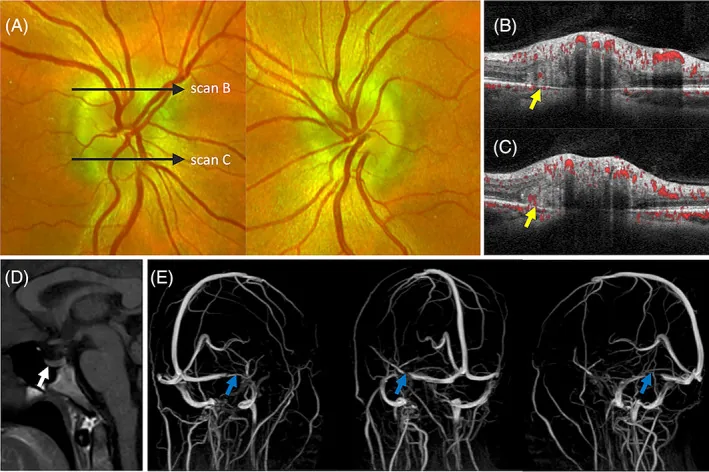
In addition to bilateral papilledema (A), OCT shows hyperreflective PHOMS with internal blood flow signals (yellow arrows) at the superior and inferior disc margins (B, C), and MRI with venography reveals optic nerve sheath distension, empty sella (white arrow, D), and transverse sinus flow defect (blue arrow, E). This corresponds to “papilledema” discussed in the section “2. Main symptoms and clinical findings”.
In the acute phase of papilledema, centripetal visual functions (best-corrected visual acuity, color vision) are usually preserved, and early subjective symptoms are often scarce.
Transient visual obscurations (TVO): Bilateral transient visual loss lasting seconds. Triggered by postural changes or Valsalva maneuver. The mechanism is thought to be transient ischemia of the optic disc.
Headache: Positional, worsening in the morning or when lying down. May be accompanied by nausea and vomiting.
Pulsatile tinnitus: A “shushing” sound. Caused by turbulent venous flow.
Diplopia: Horizontal diplopia due to abducens nerve (CN VI) palsy. Appears as a false localizing sign of increased intracranial pressure.
Visual field constriction and visual loss: When intracranial hypertension persists for months, inferonasal or concentric visual field constriction appears, followed by visual loss.
Hyperopic shift: Due to axial length shortening from flattening of the posterior globe.
In children, increased intracranial pressure is often discovered due to esotropia associated with bilateral abducens nerve palsy.
Clinical findings (findings confirmed by physician examination)
Opacity of the retinal nerve fiber layer: Loss of peripapillary sheen.
Elevation and blurring of disc margins: Margins become indistinct and the disc surface elevates.
Disc hyperemia and loss of physiologic cup: Redness and swelling of the disc, and the cup on the disc surface disappears.
Vascular changes: Dilatation and tortuosity of retinal veins, venous engorgement, hemorrhages, cotton-wool spots, exudates (may form a macular star).
Spontaneous venous pulsation (SVP): Present in about 90% of normal individuals. It disappears with increased intracranial pressure; if present, it suggests no current ICP elevation. However, note that it is absent in 10–20% of the normal population.
Paton’s lines: Concentric folds around the optic disc. May be accompanied by choroidal folds.
The severity of papilledema is assessed using the Frisén scale (stages 0–5) and used as an indicator of visual prognosis.
Stages 0–1
Stage 0 (normal): Blurring of the nasal, superior, and inferior disc margins. Radial nerve fiber layer.
Stage 1 (very early): Obscuration of the nasal disc border. No elevation of the border. Subtle grayish halo. Concentric or radial choroidal folds.
Stages 2–3
Stage 2 (early): Obscuration of all borders. Elevation of the nasal border. Complete peripapillary halo.
Stage 3 (moderate): Increased disc diameter. Obscuration of some segments of major vessels. Finger-like extensions at the outer edge of the halo.
Stages 4–5
Stage 4 (marked): Elevation of the entire disc. Complete obscuration of major vessel segments on the disc.
Stage 5 (severe): Dome-shaped protrusion. The halo is narrow with smooth borders. Disappearance of the physiologic cup.
QIf there is transient visual obscuration, does vision always worsen?
A
TVO is a characteristic symptom of papilledema, but it is not a direct precursor of vision loss. However, if intracranial hypertension persists for a long time, it can progress from severe peripheral visual field loss to central vision loss. If TVO occurs frequently, it is important to promptly see a specialist and investigate the cause.
The rate of papilledema formation depends on the rate of intracranial pressure increase. With mild, gradual ICP elevation, it may appear over several weeks; with severe, acute changes, it can appear within hours to a day.
Five mechanisms of increased intracranial pressure
Medications: Tetracycline antibiotics, vitamin A derivatives, lithium, steroids (or their withdrawal).
Genetic factors: Familial occurrence of idiopathic intracranial hypertension has been reported, and genome-wide association studies have identified candidate regions on chromosomes 5, 13, and 14, but a Mendelian inheritance pattern has not been established2).
QDoes weight loss improve papilledema?
A
When caused by idiopathic intracranial hypertension, a 5–10% weight loss has been shown to improve ICP symptoms and papilledema. However, weight management is only part of conservative treatment, and depending on the degree of papilledema and presence of visual dysfunction, combination with medication or surgical treatment may be necessary.
The diagnosis of papilledema is made through a combination of ophthalmic examination, neuroimaging, and lumbar puncture (LP). First, blood pressure is measured to rule out malignant hypertension, and emergency imaging (CT → MRI + contrast MRV) is performed to evaluate space-occupying lesions and venous sinus thrombosis. After confirming no risk of brain herniation, LP is performed.
Ophthalmoscopy: Confirmation of bilateral papilledema is fundamental. Assess redness, swelling, blurred margins, obscuration of retinal vessels, hemorrhages, exudates, and venous dilation.
Fluorescein angiography (FA): Leakage of dye from the optic disc suggests true papilledema. In pseudopapilledema, there is no leakage, only staining. However, in high myopia or buried drusen, leakage may occur even in pseudopapilledema, which is a limitation.
Optical coherence tomography (OCT) (SD-OCTretinal nerve fiber layer [RNFL]): Useful for detecting subtle disc swelling and monitoring. Ganglion cell layer-inner plexiform layer (GCL-IPL) OCT helps differentiate atrophy from improvement.
Visual field testing (automated perimetry): Evaluates enlarged blind spot, arcuate scotoma, nasal step, and concentric constriction. Humphrey 30-2 is used.
Pseudopapilledema can be caused by high hyperopia, high myopia, drusen, tilted disc, myelinated nerve fibers, hamartoma, etc. There is optic disc abnormality but no actual edema. The following findings suggest pseudopapilledema.
No telangiectasia or hyperemia on the disc surface
Absence of physiologic cupping
No hemorrhages or exudates
No retinal nerve fiber layer opacity
Blood vessels on the disc surface can be clearly traced
Malignant hypertension: Immediate emergency transport. Be aware of the combination of increased intracranial pressure and systemic hypertension (FISH).
Space-occupying lesions: Prioritize primary treatment such as surgery.
Acute cerebral venous thrombosis: Consult a specialized team in neurosurgery and neurology. Start anticoagulation therapy with warfarin. Avoid acetazolamide as it may worsen the condition. It can be considered after starting anticoagulation.
In Japan, the following are the basics of treatment for increased intracranial pressure.
Reducing intracranial pressure: Neurosurgical procedures such as removal of space-occupying lesions or ventriculoperitoneal shunt.
Idiopathic intracranial hypertension: CSF removal via lumbar puncture, administration of acetazolamide (Diamox®) or mannitol (acetazolamide is not covered by insurance in Japan).
First-line: Acetazolamide (carbonic anhydrase inhibitor). The IIHT trial supported its safety and efficacy in combination with weight loss for patients with mild visual loss, improving papilledema1). Six-month administration showed reduced ICP, improved QOL, and decreased papilledema2).
Second-line: Topiramate (anticonvulsant; lowers ICP and improves visual function)2), Furosemide (Lasix®). Used when acetazolamide is not tolerated or ineffective.
Surgical Management of Idiopathic Intracranial Hypertension
Optic nerve sheath fenestration (ONSF): Chosen when visual loss is the main problem. A small window is created in the optic nerve sheath to relieve compression2).
CSF shunting: Lumbar-peritoneal (LP) shunt is considered the primary surgical intervention for IIH2). Ventriculoperitoneal (VP) shunt is also an option. Indicated when headache is predominant, or when headache and visual loss coexist.
Dural venous sinus stenting: An option when significant venous sinus stenosis and a large pressure gradient are present. Reported to be safe and effective4).
Bariatric surgery: Surgical intervention for weight loss. The IIH Weight Trial (JAMA Neurol 2021) demonstrated its efficacy1).
Complications of surgical treatment: Shunt failure, breakage, infection; visual loss related to surgical manipulation in ONSF require attention.
Prognosis: If intracranial pressure decreases early, papilledema resolves quickly and visual function is preserved. Delayed treatment leading to visual dysfunction is irreversible. The recurrence rate of IIH is 9–28%, and regular follow-up is important2). Visual prognosis is generally good, but severe vision loss occurs in a minority2).
Poor prognostic factors: Weight gain, severity of papilledema, baseline headache severity2).
Fulminant IIH: In severe cases with profound visual loss, severe papilledema, and visual field constriction, mean CSF opening pressure can reach 54.1 cmH2O (range 29–70 cmH2O)1); 50% progress to legal blindness, and all have residual visual field defects and optic atrophy1). If baseline HVF MD is less than -7 dB, vision did not recover1).
QCan acetazolamide be used for all types of papilledema?
A
Acetazolamide is established as a first-line treatment for idiopathic intracranial hypertension, but it is contraindicated when cerebral venous thrombosis is the cause, as it may worsen the condition. It is essential to identify the underlying cause and select treatment accordingly. Note that it is used off-label in Japan.
Stasis of axoplasmic flow plays a central role in the formation of papilledema.
Mechanism of axoplasmic flow stasis:
Increased ICP behind the eye → increased pressure in the subarachnoid space around the optic nerve → compression of the optic nerve → stasis of anterograde axonal transport at the optic disc → nerve edema (papilledema).
Once atrophy occurs, dead nerve fibers do not swell, so papilledema may disappear even if ICP elevation persists (end-stage atrophy).
Pathophysiology of idiopathic intracranial hypertension: The exact mechanism is unknown. Dysregulation of CSF dynamics, metabolic and hormonal factors are thought to be involved 2). Venous sinus stenosis leading to increased venous sinus pressure and decreased CSF absorption has also been proposed. Recently, idiopathic intracranial hypertension is increasingly recognized as a systemic metabolic disorder associated with androgen dysregulation 1).
AVM-related intracranial hypertension (rare mechanism): Unruptured arteriovenous malformations (AVMs) can cause intracranial hypertension and papilledema without hemorrhage or hydrocephalus 3). The proposed mechanism is abnormal drainage due to arterialization of cortical veins → increased pulse pressure in the subarachnoid space → impaired CSF reabsorption. A literature review reported 26 such cases 3).
7. Recent Research and Future Perspectives (Investigational Reports)
Transverse sinus stenting (TSS) has been reported as a safe and effective treatment for the management of idiopathic intracranial hypertension4).
Waser et al. (2021) reported TSS in a case of papilledema with brain parenchymal herniation into the dural venous sinus (BHDVS) in a 52-year-old man4). Six months after stenting, objective resolution of papilledema and normalization of the venous sinus pressure gradient (32 mmHg → 12 mmHg, gradient >15 mmHg → 5 mmHg) were achieved.
Ghorbani et al. (2025) reported endovascular embolization in 4 cases of unruptured AVM presenting with intracranial hypertension and papilledema3). Bilateral papilledema resolved within one month after treatment, and medication adjustment was unnecessary in cases with complete embolization. In Case 1 (35-year-old man), LP opening pressure normalized from 38 cmH2O to 28 cmH2O at one week post-embolization and to 21 cmH2O at one month, with confirmed resolution of papilledema.
New concept of idiopathic intracranial hypertension as a systemic metabolic disease and treatment prospects
Idiopathic intracranial hypertension is increasingly being recognized as a systemic metabolic disease independent of obesity1). A randomized controlled trial (IIH Weight Trial, JAMA Neurol 2021) comparing bariatric surgery versus community weight management intervention demonstrated the efficacy of bariatric surgery1). Research into novel treatments targeting androgen dysregulation is ongoing1), and strengthening evidence for surgical interventions is also a priority1). Establishing the etiology, additional factors of dysfunction, and optimal treatment for idiopathic intracranial hypertension are future research challenges2).
Bonelli L, Menon V, Arnold AC, Mollan SP. Managing idiopathic intracranial hypertension in the eye clinic. Eye (London, England). 2024;38(12):2472-2481. doi:10.1038/s41433-024-03140-y. PMID:38789788; PMCID:PMC11306398.
Toshniwal SS, Kinkar J, Chadha Y, et al. Navigating the Enigma: A Comprehensive Review of Idiopathic Intracranial Hypertension. Cureus. 2024;16(3):e56256. PMID:38623134. doi:10.7759/cureus.56256.
Ghorbani M, Griessenauer CJ, Wipplinger C, et al. Intracranial hypertension and papilledema secondary to an unruptured arteriovenous malformation: review of the literature. Neuroradiol J. 2025;38(4):387-393.
Waser B, Wood HM, Mews P, Lalloo S. Transverse sinus stenting for treatment of papilloedema secondary to a large brain herniation into a dural venous sinus with associated tectal plate lesion: Case report and literature review. Interventional neuroradiology : journal of peritherapeutic neuroradiology, surgical procedures and related neurosciences. 2021;27(6):756-762. doi:10.1177/15910199211003451. PMID:33779375; PMCID:PMC8673891.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.