Orbital mucormycosis is an invasive fungal infection caused by fungi of the order Mucorales that invade the orbital tissues from the nasal cavity and paranasal sinuses. The orbital involvement in rhino-orbital-cerebral mucormycosis (ROCM) is the most important, with Rhizopus species (especially Rhizopus oryzae) accounting for approximately 85–90% of rhinocerebral cases. It was previously called orbital zygomycosis.
Mucorales fungi are highly tissue-invasive; even a small lesion can cause irreversible ocular motility disorders and vision loss if it affects the orbital apex. The estimated annual incidence is 1.7 per million people 8), and in India, the incidence is reported to be 80 times higher than in developed countries 9). In Europe, it is reported as 0.2–3 per million 4). Overall mortality exceeds 50%, reaching 79% without treatment and approximately 40.5% with treatment. Central nervous system involvement occurs in 33–49% of diabetic patients with poor glycemic control 8).
QHow often does orbital mucormycosis (rhino-orbital-cerebral mucormycosis) occur?
A
The estimated annual incidence is 1.7 per 1,000,000 people8). In India, the incidence is reported to be 80 times higher than in developed countries, showing significant regional variation. The risk is markedly increased in patients with diabetes, hematologic malignancies, or immunodeficiency. Since the COVID-19 pandemic, cases have surged, especially in India6).
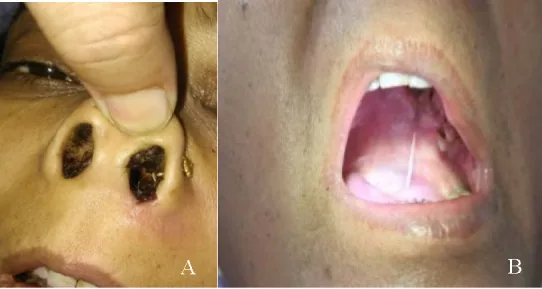
Singh SP, Rana J, Singh VK, et al. Rhino-orbital mucormycosis: Our experiences with clinical features and management in a tertiary care center. Rom J Ophthalmol. 2021;65(4):339-353. Figure 1. PMID: 35087975; PMCID: PMC8764427; DOI: 10.22336/rjo.2021.69. License: CC BY.
(A) Black necrotic eschar attached to the left nasal vestibule, (B) Clinical photograph showing necrotic lesion of the hard palate. This corresponds to the black eschar, a characteristic finding of the sinus stage discussed in the section “2. Main symptoms and clinical findings.”
In all cases of COVID-19-associated ROCM, CRAO, proptosis, and complete ophthalmoplegia were observed, and the prognosis was extremely poor (all cases died)3).
Fungi of the order Mucorales, particularly Rhizopus oryzae, are the main causative organisms. They are fast-growing, aseptate filamentous fungi that are widely distributed in tropical and subtropical regions. They invade the body through inhalation of spores.
Diabetes mellitus (especially diabetic ketoacidosis): The greatest risk factor (58.9–86.7%)
Hematologic malignancies (e.g., acute myeloid leukemia) and neutropenia
History of kidney transplantation and immunosuppressive therapy
HIV infection, chronic kidney disease, and malnutrition
Hemochromatosis and deferoxamine therapy
COVID-19 infection: Risk increases especially with steroid use and diabetes comorbidity6)7)
Prolonged ICU stay and intravenous drug use
Voriconazole prophylaxis (may induce overgrowth of Mucorales)4)
QDoes COVID-19 increase the risk of mucormycosis?
A
Cases of ROCM after COVID-19 infection have increased rapidly worldwide, with 2,826 cases reported in India in 2021 alone 6). The cytokine storm, immune abnormalities, steroid use, and hyperglycemia caused by COVID-19 are thought to synergistically promote fungal growth.
Passi N, Wadhwa AC, Naik S. Radiological spectrum of invasive mucormycosis in COVID-19. BJR Case Rep. 2022;7(6):20210111. Figure 4. PMID: 35300232; PMCID: PMC8906162; DOI: 10.1259/bjrcr.20210111. License: CC BY.
Non-contrast coronal CT of the sinuses. Opacification of the ethmoid and maxillary sinuses, bone erosion of the sinus wall (arrowhead), and soft tissue infiltration into the orbit reaching the medial rectus muscle (arrow) with loss of the fat plane. Corresponds to CT findings (bone erosion, orbital extension) discussed in the section “4. Diagnosis and Testing Methods.”
CT: Useful for evaluating bone erosion and opacification of the sinus walls. The most commonly involved sites are the maxillary and ethmoid sinuses. Contrast-enhanced CT is preferred. Many cases show no abnormalities in the early stage, so repeated imaging is important. Pay attention to findings of sinusitis near the lesion (mucosal thickening, opacification).
Biopsy and culture are the gold standard for definitive diagnosis. Histopathology uses H&E, PAS, and GMS staining, with characteristic findings including broad, ribbon-like, non-septate hyphae branching at right angles (90 degrees), vascular invasion, thrombosis, and necrosis 2). Identification of the fungal species by culture is important for selecting treatment, but the culture positivity rate is low. Definitive diagnosis is made by demonstrating the organism through histopathological examination or culture.
DNA sequences of Rhizopus species can be detected in cerebrospinal fluid. Positivity was reported in all 7 cases (all cultures were negative), making it particularly useful when conventional methods are negative.
The characteristics of diagnostic methods are shown below.
Test Method
Features
Cautions
Biopsy + Culture
Gold standard for definitive diagnosis
Low culture positivity rate
mNGS (CSF)
Detectable even in culture-negative cases
Requires specialized facilities
β-D-glucan / GM
Routine fungal markers
Low sensitivity for Mucorales, unsuitable for diagnosis
The combination of antifungal drugs and surgical debridement is the standard, and treatment in an internal medicine department capable of systemic management is desirable. Since antifungal drug penetration into necrotic tissue is poor, combination with surgical treatment is essential.
Usually 5–7.5 mg/kg/day; 10 mg/kg/day for CNS involvement
Posaconazole
Step-down/salvage therapy
Response rate 60–70%2)
Isavuconazole
Alternative therapy (well tolerated) 7)
200 mg loading dose, then 200 mg/day (oral)
Voriconazole
Ineffective for mucormycosis
Not usable (critical difference from aspergillosis)
First-line: liposomal amphotericin B (L-AMB)2)
Usual dose: 5–7.5 mg/kg/day
CNS involvement: 10 mg/kg/day 1)
Duration: 3–36 months (based on clinical and imaging improvement)
Amphotericin B deoxycholate has significantly higher nephrotoxicity; liposomal formulation is preferred
Posaconazole: step-down or salvage therapy. Response rate 60–70% 2).
Isavuconazole: effective as alternative therapy, well tolerated 7). 200 mg loading dose, then 200 mg/day (oral).
Combination therapy: amphotericin plus caspofungin has been reported to have better outcomes than monotherapy, but echinocandins have low in vitro activity against Mucorales, and strong evidence is lacking 2).
Surgical debridement of necrotic tissue is essential. Resection should be performed until normal bleeding is obtained, and pathological confirmation of the resection margins is strongly recommended. Functional endoscopic sinus surgery (FESS) is the standard procedure, and multiple surgeries may be required 4). Otolaryngological treatment of the sinuses is often necessary in adults, and it is particularly important to reduce intraorbital pressure when visual acuity is decreased. In cases with extensive orbital involvement, orbital exenteration with bone removal may be necessary.
The mortality rate for antifungal therapy combined with surgery is 18.5%, whereas it is significantly higher at 60% for antifungal therapy alone 2).
Blood glucose control in diabetes and correction of diabetic ketoacidosis 7)
Correction of immunosuppressive state (reduction of immunosuppressive drugs as much as possible)
QHow long does treatment take?
A
The duration of liposomal amphotericin B administration ranges from 3 to 36 months, adjusted individually according to clinical and imaging improvement 2). Severe cases or those with cerebral extension often require longer administration. Surgical debridement may also need to be performed multiple times.
QIs voriconazole ineffective against mucormycosis?
A
Voriconazole is an effective antifungal drug for aspergillosis, but it is ineffective against mucormycosis (Mucorales). Since both can present with similar symptoms and findings, identification of the causative organism is extremely important for treatment selection. Cases of breakthrough mucormycosis infection during voriconazole administration have been reported 4), making reliable fungal identification necessary.
Spores are inhaled and proliferate in the paranasal sinuses, reaching the orbit via direct invasion or through the nasolacrimal duct. From the orbit, they invade the brain through the orbital apex, cavernous sinus, cribriform plate, and blood vessels.
The main spread mechanism is angioinvasion, penetrating the endothelial cells of blood vessel walls and extracellular matrix proteins. GRP78 (glucose-regulated protein) is involved in this penetration process. Progression occurs via angioinvasion → thrombosis → ischemia → avascular necrosis, forming necrosis without congestion.
Under acidic conditions, iron is released from transferrin, and Mucorales fungi utilize free iron to proliferate rapidly. A similar mechanism occurs in iron overload states (hemochromatosis, frequent blood transfusions, deferoxamine therapy).
Cytokine storm (elevation of IL-1, IL-2, IL-6, TNF-α, etc.), decreased IFN-γ expression in CD4+ T cells, use of steroids and immunomodulators, and the overlap of hypoxic environment + hyperglycemia + acidic environment + high iron levels provide an ideal environment for fungal spore germination 7).
Yang et al. (2026) reported 7 cases of ROCM presenting with cerebral infarction as the initial symptom 5). In all cases, Rhizopus species were detected by mNGS of cerebrospinal fluid, but cultures were negative in all cases. The median time to diagnosis was 5 days, and the only survivor was diagnosed within 2 days (mortality rate 85.7%). mNGS is a promising early diagnostic tool for ROCM, especially valuable when conventional cultures and serum markers are negative.
QIn what situations is mNGS testing useful?
A
mNGS (metagenomic next-generation sequencing) is useful when β-D-glucan and galactomannan have poor sensitivity and cultures fail to identify the causative organism. Particularly in atypical ROCM presenting with cerebral infarction as the initial symptom, CSF mNGS may be the only diagnostic method 5).
Rapid Increase in COVID-19-Associated ROCM and Countermeasures
In response to the global surge in ROCM complicating COVID-19, Ostovan et al. (2021) reported that all patients with a history of mechanical ventilation died 6). In India, Sen et al. (2021) reported 2,826 cases of COVID-19-associated ROCM, drawing attention as a new serious complication of the pandemic.
Al Reesi et al. (2023) reported a case of pediatric ROCM with acute chronic kidney disease and malnutrition that was cured with aggressive treatment including liposomal amphotericin B (5→9 mg/kg/day) + posaconazole + multiple surgeries 2). Early diagnosis within 24 hours and aggressive treatment are considered key to favorable outcomes.
Benlamkaddem S, Zdaik G, Doughmi D, Bennis A, Chraibi F, Berdai MA, et al. Rhino-Orbital Cerebral Mucormycosis: A Fatal Evolution. Cureus. 2023;15(4):e37837. doi:10.7759/cureus.37837. PMID:37214071; PMCID:PMC10198304.
Al Reesi M, Al Muqbali T, Al Ajmi A, et al. Successful Management of Rhino-Orbital-Cerebral Mucormycosis in a Child with Acute-on-Chronic Kidney Disease and Malnutrition. Sultan Qaboos Univ Med J. 2023.
Kamath GM, Jeganathan S, Salim S, Antony RM, Kamath AR, Hiran H. Case series of central retinal artery occlusion in COVID-19-associated rhino-orbital-cerebral mucormycosis. Indian journal of ophthalmology. 2023;71(7):2904-2906. doi:10.4103/IJO.IJO_3123_22. PMID:37417144; PMCID:PMC10491029.
Siriwardena P, Wariyapperuma U, Nanayakkara P, Jayawardena N, Mendis D, Bahar M, et al. Rhino-orbital-cerebral mucormycosis in acute myeloid leukemia patients: a case series from Sri Lanka. BMC infectious diseases. 2024;24(1):1465. doi:10.1186/s12879-024-10334-y. PMID:39725915; PMCID:PMC11670406.
Yang F, Yang C, Li H, Zhang X, Ding X, Zhang S. Metagenomic next-generation sequencing in diagnosing rhino-orbital-cerebral mucormycosis presenting as cerebral Infarction: a case series and diagnostic analysis of seven patients. Frontiers in fungal biology. 2026;7:1751546. doi:10.3389/ffunb.2026.1751546. PMID:41659795; PMCID:PMC12873710.
Ostovan VR, Rezapanah S, Behzadi Z, Hosseini L, Jahangiri R, Anbardar MH, et al. Coronavirus disease (COVID-19) complicated by rhino-orbital-cerebral mucormycosis presenting with neurovascular thrombosis: a case report and review of literature. Journal of neurovirology. 2021;27(4):644-649. doi:10.1007/s13365-021-00996-8. PMID:34342852; PMCID:PMC8330178.
Ponce-Rosas L, Gonzales-Zamora J, Diaz-Reyes N, et al. Rhino-Orbital-Cerebral Mucormycosis in a Post-COVID-19 Patient from Peru. Case Rep Infect Dis. 2022.
Alanazi RF, Almalki A, Alkhaibary A, AlSufiani F, Aloraidi A. Rhino-Orbital-Cerebral Mucormycosis: A Rare Complication of Uncontrolled Diabetes. Case reports in surgery. 2022;2022:6535588. doi:10.1155/2022/6535588. PMID:36245688; PMCID:PMC9556216.
Mokhtar EA, Fatima Q, Akbar S, Equbal S, Salahudeen A. Rhino-Orbital Cerebral Mucormycosis Causing Temporomandibular Joint Ankylosis: A Case Series of Two Patients. Cureus. 2023;15(2):e35194. doi:10.7759/cureus.35194. PMID:36960262; PMCID:PMC10030649.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.