Polyarteritis nodosa (PAN) is a systemic necrotizing vasculitis that primarily affects medium-sized arteries. It causes inflammation in all layers of the arterial wall and perivascular inflammatory cell infiltration, leading to fibrinoid necrosis.
The incidence is 0.7 per 100,000 person-years in biopsy-confirmed cases, and the prevalence is 6.3 per 100,000, making it a rare disease. A report from a multi-ethnic population in France found a prevalence of 33 per million and an incidence of 0 to 1.6 per year 1). It typically occurs between 40 and 60 years of age, with a slight male predominance (male-to-female ratio 1.5:1) 1).
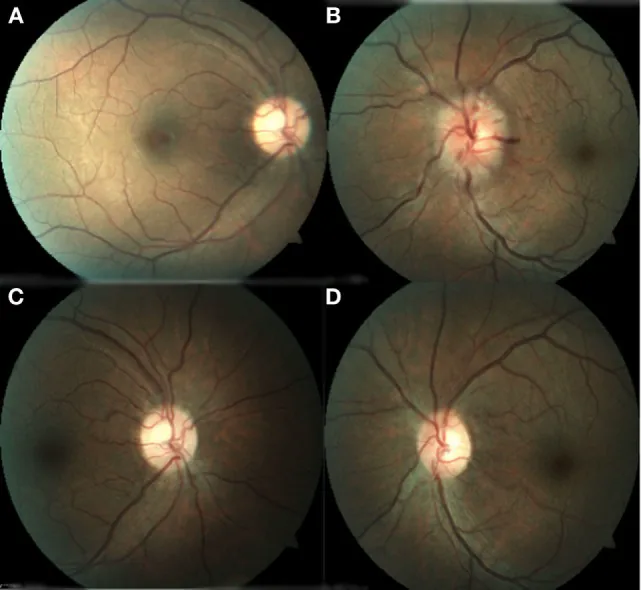
Among systemic symptoms, neurological symptoms are frequent, occurring in 79% of 348 cases in Pagnoux 2010 1). Ocular involvement occurs in 9–20% of cases, presenting various neuro-ophthalmic signs such as choroidal vasculitis, retinal vascular occlusion, ischemic optic neuropathy, and cranial nerve palsy. One characteristic of this disease is that lung involvement is generally absent.
There is an association with hepatitis B virus (HBV); currently, HBV-related PAN accounts for 7–10% of all cases. Before the widespread use of the HBV vaccine, it accounted for 36%, but this decreased after vaccination became common.
QHow often does PAN affect the eyes?
A
Ocular involvement occurs in 10–20% of patients. Choroidal vasculitis is the most common ocular finding, and multifocal acute ischemia of the choriocapillaris strongly suggests vasculitis. The frequency of involvement is even higher when neuro-ophthalmic findings (e.g., cranial nerve palsy, homonymous hemianopia) are included.
Kristian A Vazquez-Romo, Adrian Rodriguez-Hernandez, Jose A Paczka et al. Optic Neuropathy Secondary to Polyarteritis Nodosa, Case Report, and Diagnostic Challenges. Frontiers in Neurology. 2017 Sep 20; 8:490. Figure 1. PMCID: PMC5611380. License: CC BY.
Caption describing the image of PAN ocular findings
The pathophysiology of PAN is not fully understood. Genetic predisposition triggered by environmental stimuli is suspected.
The basic pathology involves immune complex deposition in the walls of medium-sized arteries, leading to necrosis. Fibrinoid necrosis occurs in small and medium-sized arteries.
The main risk factors and related factors are as follows.
HBV infection: Strong association with PAN, often developing within 6 months of infection. The mechanism involves serum immune complex deposition and complement consumption. After the spread of HBV vaccine, HBV-related PAN decreased from 36% in the 1970s to 7%.
HCV infection: Although not as strong as HBV, an association has been reported.
CECR1 mutation (DADA2): Causes adenosine deaminase 2 (ADA2) deficiency, with earlier onset (mostly by age 10) and higher frequency of stroke.
Drugs: Long-term use of minocycline for more than 3 years has been reported to cause renal PAN. In some cases, aneurysms disappeared with drug discontinuation alone 3).
COVID-19 mRNA vaccine: Four cases of onset within 7 to 28 days after vaccination have been reported 5).
Others: Associations with parvovirus B19, CMV, EBV, HIV infection, hairy cell leukemia, and VEXAS syndrome have also been reported 1).
According to the criteria of the Ministry of Health and Welfare Research Group on Intractable Vasculitis (1998), a definite case is defined as having at least 2 of the following 10 major symptoms, along with angiographic findings or pathological findings of vasculitis.
Fever (38°C or higher for 2 weeks or more) and weight loss (6 kg or more within 6 months)
Hypertension
Progressive renal failure
Cerebral infarction (hemorrhage)
Ischemic heart disease, pericarditis, or heart failure
Pleurisy
Gastrointestinal bleeding or intestinal obstruction
ANCA: Classic PAN is usually negative. MPO-ANCA may be positive in 10%, but positive cases should consider microscopic polyangiitis (MPA). High ANCA significantly reduces the likelihood of PAN.
Viral testing: Check HBV, HCV, and HIV serology.
IL-6: Correlates with disease activity; high levels tend to be associated with arthralgia and skin ulcers 2).
QIs there a specific blood test for the definitive diagnosis of PAN?
A
There is no single test that confirms PAN. Nonspecific inflammatory findings such as elevated ESR and CRP are observed, while ANCA and cryoglobulins are usually negative, which can be a clue. Confirmation of HBV, HCV, and HIV serology is also essential. Definitive diagnosis requires angiography or tissue biopsy.
Fluorescein angiography (FA): Useful for visualizing multifocal acute ischemia of the choriocapillaris. Prolonged arm-to-retina and retinal circulation times are observed.
Head MRI: Multiple scattered lesions in the cortex and subcortex (gray and white matter). Gadolinium-enhanced FLAIR images can confirm the coexistence of small hemorrhagic lesions and multiple infarcts.
MRA/CTA: Depicts multiple microaneurysms (1–5 mm) and coexisting stenotic lesions in the mesenteric, renal, and hepatic arteries. The alternating appearance of arterial stenosis and aneurysmal dilation is a characteristic finding6).
Visceral angiography: Performed when biopsy is negative or when visceral symptoms are predominant. Focal segmental aneurysms in the mesenteric, hepatic, and renal arteries are confirmed in up to 90% of cases1).
QWhat should be noted in ophthalmologic follow-up of PAN patients?
A
Attention should be paid to opportunistic infections such as CMV retinitis during immunosuppressive therapy, steroid-induced central serous chorioretinopathy, and neovascularization from retinal non-perfusion areas. Regular fundus examinations including fluorescein angiography are recommended.
The basic lesion of PAN is transmural inflammation of the walls of medium-sized arteries.
The inflammatory cascade is thought to progress as follows.
Initiation of endothelial injury: Direct injury or cytokine/antibody-mediated endothelial damage occurs triggered by environmental stimuli (infection, drugs, etc.).
Release of inflammatory cytokines: IL-2, IL-8, and IFN-γ become elevated, and leukocytes are recruited to the arterial media.
Destruction of the internal elastic lamina: Neutrophil infiltration destroys the internal elastic lamina, causing intimal thickening, edema, and thrombosis.
Arterial occlusion and aneurysm formation: Occlusion due to thrombosis and aneurysm formation due to weakening of the arterial wall coexist. The coexistence of both on angiography is a typical finding of PAN.
In HBV-associated PAN, immune complex deposition and complement consumption are the main mechanisms of arteritis.
Weakening of CNS arteries leads to aneurysm formation, which can rupture and cause hemorrhagic infarction. Chronic inflammation leads to stenosis and thrombosis, causing ischemic lesions. In the eye, impaired blood flow to the choroid, retina, and optic nerve produces various ocular findings.
In DADA2 (CECR1 mutation), ADA2 deficiency is thought to cause overactivation of M1 macrophages, promoting inflammation and destruction of the vessel wall.
In a report by Boistault et al. (2021), a refractory pediatric PAN case showed markedly elevated IL-6 at 106.43 pg/mL (normal 0–4.3 pg/mL)2). The high IL-6 group was predominantly male and showed significantly more joint pain and skin ulcers.
7. Latest Research and Future Prospects (Research-stage Reports)
The application of tocilizumab (TCZ), an IL-6 receptor inhibitor, to refractory PAN has been reported.
Boistault et al. (2021) summarized 11 cases of refractory PAN (median age 35 years, IQR 23.5–57.5 years, 5 female) treated with TCZ2). The dose was TCZ 8 mg/kg intravenously every 2–4 weeks or TCZ 162 mg subcutaneously weekly, and remission was achieved in most cases.
In one case of childhood PAN, a 4-year-old girl refractory to high-dose steroids plus cyclophosphamide was started on TCZ 8 mg/kg every 2 weeks, resulting in clinical and biological improvement within days, and complete remission was maintained at 21 months2). The rationale for choosing TCZ was that IL-6 levels were relatively higher than TNF-α.
Four cases of PAN onset after COVID-19 mRNA vaccination have been reported.
Ohkubo et al. (2022) summarized cases of PAN onset within 7–28 days after vaccination5). Most cases occurred after the first dose, and all improved with steroids and immunosuppressants. The proposed mechanism involves an inflammatory reaction to lipid nanoparticle (LNP) injection, leading to neutrophil infiltration and inflammatory cytokine production.
A causal relationship has not been established, and the benefits of vaccination are considered to greatly outweigh the risks.
Non-immunosuppressive management of drug-induced PAN
Yokota et al. (2022) reported the first case in the English literature where renal PAN developed after taking minocycline for more than 3 years, and functional and morphological remission was achieved by drug discontinuation alone 3). Repeat angiography after 7.5 years confirmed the disappearance of renal artery aneurysms, and the patient was managed without steroids or immunosuppressants.
In drug-induced PAN, discontinuation of the causative drug is the highest priority, and this finding is important as it shows the possibility of achieving remission without immunosuppressive therapy.
Ambrogetti R, Taha O, Awan B, et al. Pericarditis of Polyarteritis Nodosa. Cureus. 2023;15(10):e46717.
Boistault M, Lopez Corbeto M, Quartier P, et al. A young girl with severe polyarteritis nodosa successfully treated with tocilizumab: a case report. Pediatr Rheumatol Online J. 2021;19:168.
Yokota K, Kurihara I, Nakamura T, et al. Remission of Angiographically Confirmed Minocycline-induced Renal Polyarteritis Nodosa: A Case Report and Literature Review. Intern Med. 2022;61:103-110.
Waisayarat J, Niyasom C, Vilaiyuk S, Molagool S. Polyarteritis Nodosa with Cytomegalovirus Enteritis and Jejunoileal Perforation: Report of a Case with a Literature Review. Vascular health and risk management. 2022;18:595-601. doi:10.2147/VHRM.S354548. PMID:35924006; PMCID:PMC9342704.
Ohkubo Y, Ohmura S, Ishihara R, et al. Possible case of polyarteritis nodosa with epididymitis following COVID-19 vaccination: A case report and review of the literature. Mod Rheumatol Case Rep. 2022;(epub).
Robinson C, Yasin Z, Patel P, et al. A Rare Presentation of Polyarteritis Nodosa. Cureus. 2022;14(2):e21925.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.