Non-arteritic
Optic disc findings: Normal in the acute phase. Pallor develops after 6–8 weeks.
Visual acuity: 20/200 or worse in 69%.
Course: Rare onset. Steroid therapy has been reported to improve visual fields.

Posterior Ischemic Optic Neuropathy (PION) is an ischemic optic neuropathy caused by circulatory insufficiency in the optic nerve posterior to the lamina cribrosa. It is clearly distinguished from anterior ischemic optic neuropathy (AION) by the absence of optic disc swelling in the acute phase. Anterior ischemic optic neuropathy (AION) presents with disc swelling in the acute phase and is classified into arteritic (AAION) and non-arteritic (NAION) types based on etiology. NAION is essentially always anterior, while arteritic PION is classified as posterior (PAION).
PION is a rare disease accounting for only about 10% of all optic nerve ischemia cases, and it occurs more frequently after age 50. It is classified into the following three types:
The main difference is the optic disc appearance in the acute phase. In AION, disc swelling occurs acutely, whereas in PION, the disc appears normal in the acute phase, and pallor (atrophy) appears 6 to 8 weeks later. The site of ischemia is anterior to the lamina cribrosa in AION and posterior to the lamina cribrosa in PION.
It varies greatly by type. In non-arteritic PION, 69% of cases have visual acuity of 20/200 or worse, and only 20% maintain 20/40 or better. In perioperative PION, the most common final visual acuity is no light perception (NLP), and 75.8% of eyes have counting fingers or worse. 1)
Non-arteritic
Optic disc findings: Normal in the acute phase. Pallor develops after 6–8 weeks.
Visual acuity: 20/200 or worse in 69%.
Course: Rare onset. Steroid therapy has been reported to improve visual fields.
Arteritic (giant cell arteritis)
Optic disc findings: Normal in the acute phase. Pallor develops later.
Systemic symptoms: Accompanied by headache, jaw claudication, and elevated ESR/CRP.
Course: Visual recovery is less likely than in non-arteritic PION.
Perioperative
Onset pattern: Noticed upon awakening or within a few days after surgery.
Affected side: Bilateral in 70%.
Course: Most severe. NLP is the most common outcome.
Secondary to microvascular disease, involving the following vascular risk factors.
Occurs in younger patients than arteritic PION. The following risk factors are known.
Pre-existing risk factors:
Intraoperative risk factors:
Associated surgical procedures (in order of frequency):
The incidence after spinal surgery is reported as 0.087%, and after neck dissection as 0.08%.1)
The incidence after spinal surgery is reported as 0.087%, and after neck dissection as 0.08%.1) Although the frequency is low, the visual prognosis is extremely poor once it occurs, so preoperative explanation and perioperative management for high-risk patients are important.
PION is a clinical diagnosis and also a diagnosis of exclusion. The diagnostic process is as follows.
The process involves: acute vision loss + visual field defect + positive RAPD + normal optic disc findings in the acute phase → optic disc pallor after 6–8 weeks → exclusion of other causes (retrobulbar optic neuritis, retinal disease, compression, toxicity, etc.). Perioperative PION is relatively straightforward to diagnose because vision loss occurs after non-ophthalmic surgery.
In patients aged 50 years or older, measure ESR and CRP to rule out giant cell arteritis.
The sensitivity and specificity of each test for diagnosing giant cell arteritis are shown below.
| Test | Sensitivity | Specificity |
|---|---|---|
| ESR + CRP combined | Up to 100% | 97% |
| Thrombocytosis | 57.0% | 96.5% |
| Low hemoglobin | 46.3% | 92.9% |
| Decreased hematocrit | 39.8% | 91.3% |
| Leukocytosis | 28.1% | 85.7% |
CRP has higher specificity than ESR. The reference value for ESR is half of age for men and half of (age + 10) for women. Temporal artery biopsy (TAB) is the gold standard for diagnosing giant cell arteritis, with sensitivity and specificity both over 95% when performed properly. Biopsy should be performed within a few days even after starting steroid treatment. In non-arteritic PION, these test values are normal.
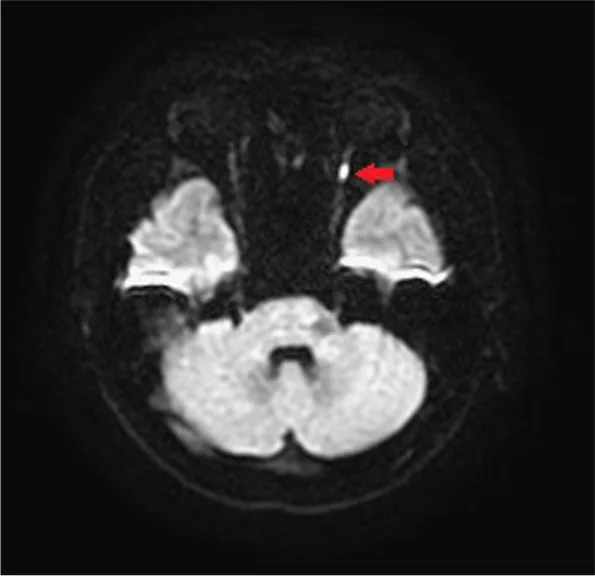
The main differential diagnoses include retrobulbar optic neuritis, macular/retinal diseases, toxic optic neuropathy, and compression or inflammation of the posterior optic nerve. To differentiate ischemic optic neuropathy from retrobulbar optic neuritis, VEP, electroretinography, OCT, and DWI MRI are used in combination.
The following protocol is recommended:
According to overseas reports, the median initial dose is prednisolone 80 mg/day, which is tapered after ESR and CRP stabilize. The total treatment duration including tapering is approximately 2.5 months.
No established effective treatment exists. Anticoagulation therapy, vasodilators, oral steroids, and optic nerve sheath decompression have been attempted, but no significant improvement in visual prognosis has been demonstrated. A regimen of prednisolone 80 mg/day for 2 weeks followed by tapering may be considered, but no RCT data are available.
No established treatment exists. Steroids are generally not recommended. General measures include:
Practice Advisory for Spinal Surgery (Perioperative Management Guidelines)
Systematic preoperative, intraoperative, and postoperative management is important for preventing vision loss.
Preoperative:
Intraoperative:
Postoperative:
Prognosis varies greatly by subtype. In arteritic PION, immediate steroid administration can reduce progression and fellow eye involvement, but significant improvement in already reduced vision is unlikely. Perioperative PION does not respond to steroids and often follows a bilateral, irreversible, and severe course. For non-arteritic PION, some reports show visual field improvement with steroids, but there is no established evidence.
The posterior optic nerve is divided into three segments: intraorbital, intracanalicular, and intracranial. The retrolaminar optic nerve receives blood supply from the pial vascular plexus and branches of the central retinal artery.
Postoperative hemorrhage and increased intracranial pressure due to bilateral internal jugular vein (IJV) compression reduce optic nerve perfusion, contributing to the development. 1) IJV ligation has been suggested as a risk factor for ischemic optic neuropathy, and impaired arterial perfusion due to venous congestion is assumed. 1) The mechanisms of reduced oxygen supply include: ① low oxygen levels in circulating blood, ② decreased arterial perfusion pressure, and ③ increased blood flow resistance. 1)
Kohyama et al. (2022) reported a case of PION that developed after laryngopharyngectomy with bilateral neck dissection and free jejunal flap reconstruction. 1) This is considered the first reported case of PION caused by postoperative hemorrhage and bilateral IJV compression.
Surgery time 13.5 hours, total blood loss 740 g. Systolic blood pressure dropped from approximately 150 mmHg preoperatively to a minimum of 80 mmHg (for several minutes). Hemoglobin decreased from 13.5 g/dL preoperatively to 9.5 g/dL postoperatively, then dropped sharply to 6.1 g/dL due to hemorrhage. Hematocrit decreased from 38.1% preoperatively to 29.3% postoperatively, then dropped to 19.3%. Postoperatively, facial and neck edema occurred, and both IJVs were compressed by hematoma. 1)
Oral prednisolone at 1 mg/kg/day was administered for more than 2 months, but visual acuity remained at the level of light perception without improvement, and no visual recovery was observed even after 1 year. 1) There was a 7-hour delay from the onset of edema to the release of the hematoma, and the authors suggest that early exploratory incision might have prevented PION. 1) It has also been reported that 75.8% of eyes with perioperative PION have visual acuity of counting fingers or worse. 1)
Regarding steroid therapy for non-arteritic PION, significant improvement in visual field (P=0.030) was observed in the steroid-treated group compared to the control group, and significant improvements in visual field (P<0.001) and visual acuity (P=0.031) were also reported relative to baseline. However, no RCT data are available.
There are reports that the combination of hyperbaric oxygen therapy within 72 hours of onset and steroids was successful in a small number of cases of perioperative PION. Further case accumulation and research are awaited.