Arteritic anterior ischemic optic neuropathy (AAION) is caused by optic nerve ischemia due to vasculitis of the nutrient vessels. Vasculitis leads to narrowing of the vascular lumen and thrombus formation due to vessel wall thickening, resulting in ischemic necrosis. Vasculitis of the short posterior ciliary arteries (SPCAs), which supply the optic disc, is considered the underlying cause. AAION accounts for 5–10% of all anterior ischemic optic neuropathy cases; the majority are non-arteritic anterior ischemic optic neuropathy (NAION).
The most common underlying disease is giant cell arteritis (GCA, formerly temporal arteritis). Other causes include herpes zoster, relapsing polychondritis, Takayasu arteritis, rheumatoid arthritis, polyarteritis nodosa, SLE, and allergic granulomatous angiitis (Churg-Strauss syndrome).
Overview and History of Giant Cell Arteritis (GCA)
GCA is a systemic granulomatous vasculitis affecting medium to large arteries. The earliest description is attributed to Ali Ibn Isa al-Kahhal of 10th-century Baghdad. In 1890, Hutchinson described red streaks with head pain, and in 1932, Bayard Horton performed the first temporal artery biopsy, describing granulomatous vasculitis. In 1941, Gilmour first described giant cells, establishing the current name.
It is more common in women over 50 years old (male-to-female ratio 1:3), and the incidence increases sharply after age 70. The median age of onset of GCA is 75 years. The estimated annual incidence of AAION in people over 50 is 0.36 per 100,000.
Visual complications of GCA occur in 10–30% (up to 70% in some reports), and AAION accounts for 60–90% of vision loss associated with GCA 3). The incidence of GCA increases with age, reaching 2.3 per 100,000 in the 60s and 44.7 per 100,000 in the 90s.
It is most common in Northern European Caucasians (about 30 per 100,000 in Norway) and rare in Black and Asian populations. The incidence in Japan is 1.47 per 100,000, which is extremely rare compared to Western countries. In Europe, it is the most common primary systemic vasculitis in people over 50, with an annual incidence of 32–290 per million 6).
QHow is AAION different from non-arteritic anterior ischemic optic neuropathy (NAION)?
A
AAION accounts for 5–10% of all anterior ischemic optic neuropathies and is caused by vasculitis such as giant cell arteritis. Visual prognosis is significantly worse than NAION, with more than 60% having visual acuity less than 20/200. In NAION, a “disc at risk” (small optic disc with small cup) is seen in the fellow eye, but in AAION, the contralateral disc diameter and physiological cup are normal. Inflammatory markers such as ESR and CRP are useful for differentiation, and these are not elevated in NAION.
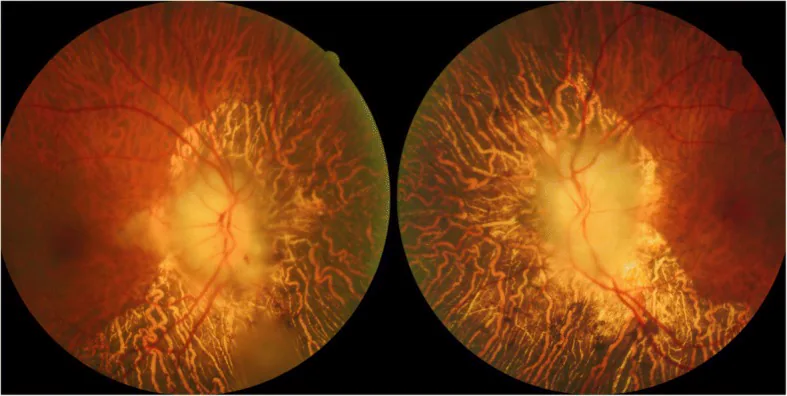
Tian G, et al. Giant cell arteritis presenting as bilateral anterior ischemic optic neuropathy: a biopsy-proven case report in Chinese patient. BMC Ophthalmol. 2018. Figure 1. PMCID: PMC6208180. License: CC BY.
Fundus photograph at initial presentation showing severe bilateral optic disc edema with a chalky white appearance, linear hemorrhages and soft exudates in the right eye, and diffuse peripapillary choroidal atrophy. This corresponds to the “chalky white edema” discussed in the section “2. Main symptoms and clinical findings.”
In GCA, elderly patients present with acute unilateral or bilateral vision loss. Many patients experience transient monocular vision loss as a prodromal symptom. Without treatment, the fellow eye is frequently affected within a short period.
Acute vision loss: More than 60% develop severe impairment with visual acuity less than 20/200. Over 20% progress to no light perception, a severe visual dysfunction.
Transient monocular vision loss: Occurs as a prodromal symptom in about 30% of permanent vision loss cases, with an average onset 8.5 days prior. Reported incidence is 2–19%. It is extremely rare in NAION and is an important differentiating feature.
Headache: The most common systemic symptom, occurring in 65–90% of cases. New-onset temporal or occipital headache is characteristic 1).
Jaw claudication: Pain or fatigue in the jaw during chewing. This is the most specific symptom of GCA. Frequency is 11–45% 1).
Scalp tenderness: Tenderness over the temporal artery or scalp area. Discomfort occurs when combing hair or resting the head on a pillow.
Systemic symptoms: fever, weight loss, malaise, anorexia, myalgia, arthralgia, etc.
PMR (polymyalgia rheumatica) symptoms: occurs in up to 50% of patients. Presents with bilateral pain and stiffness in the neck, shoulders, and pelvis.
Diplopia: due to cranial nerve III, IV, or VI palsy. Occurs in 10–15% of cases3).
Limited eye movement: may result from cranial nerve palsy.
Occult GCA: up to 20% of AAION patients lack obvious systemic symptoms.
QIs AAION possible even without systemic symptoms?
A
Yes. A condition called occult giant cell arteritis (occult GCA) is present in up to 20% of AAION patients and lacks typical systemic symptoms such as headache and jaw claudication. The absence of systemic symptoms does not rule out giant cell arteritis; evaluation with blood tests (ESR, CRP) and temporal artery biopsy is essential.
Clinical findings (findings confirmed by physician examination)
Fluorescein angiography: Delayed filling of the optic disc and peripapillary choroid, with segmental filling defects (segmental ischemia) characteristic.
In vasculitis, thickening of the vessel wall leads to luminal narrowing and thrombosis, causing ischemic necrosis. Vasculitis of the short posterior ciliary arteries (SPCAs) causes anterior optic nerve ischemia, also accompanied by segmental choroidal ischemia.
The direct ocular mechanisms are as follows:
Inflammation of the short posterior ciliary arteries → vessel wall thickening → luminal narrowing → thrombosis → optic disc ischemia.
Occlusion of the medial SPCA is most common (particularly affected in 20% of cases).
SPCAs supply the prelaminar and laminar regions and also contribute to the peripapillary choroidal circulation.
Dendritic cells in the vessel wall act as key contributors to the disease. Macrophages and T cells invade through the vasa vasorum of the adventitia, initiating a pathogenic cascade that leads to granulomatous vasculitis affecting medium to large arteries.
Age: The greatest risk factor. Median age 75 years. Onset under 50 years is extremely rare.
Sex: Women have 2 to 6 times higher risk.
Race: Most common in Northern European Caucasians. Rare in Black and Asian populations.
Genetic factors: HLA-DRB1*04, DRW6, and DR3 are associated with increased susceptibility. Polymorphisms in the TNF-α gene locus and IL-10 promoter also correlate with increased risk. Familial GCA has been reported in non-Caucasians 7).
Environmental and infectious factors: Involvement of varicella-zoster virus (VZV), Chlamydia pneumoniae, and parvovirus B19 has been suggested.
Age-related mechanisms: Calcification of the internal elastic lamina, elastin, and extracellular matrix may explain age-specific expression.
Smoking, low BMI, early menopause: All reported as risk factors.
PMR association: GCA and PMR show a strong association.
COVID-19: Some reports indicate a 70% increase in GCA incidence during the pandemic 2). SARS-CoV-2 has affinity for vascular endothelium, and similarity to vasculitis suggests a pathological link.
Diagnosis of AAION is carried out in parallel with the definitive diagnosis of giant cell arteritis. Since differentiation between AAION and NAION directly affects treatment strategy, rapid and systematic evaluation is important.
ESR: Sensitivity 86%. May reach 70–120 mm/h. Normal reference: men = age/2, women = (age+10)/2. However, up to 10% show normal values.
CRP: Sensitivity 97.5%. Higher specificity than ESR. In the 2022 ACR/EULAR classification criteria, CRP ≥10 mg/L was added as an item 4).
ESR+CRP combined: Sensitivity 99.2%, specificity 97%. Acute phase reactants are elevated in over 80% of cases.
Others: Thrombocytosis, and the combination of CRP and platelets, has the highest diagnostic utility (p<0.001) 4).
Temporal Artery Biopsy (TAB)
Role: Gold standard for definitive diagnosis of giant cell arteritis. When performed appropriately, sensitivity and specificity are both over 95%.
Positive findings: Intimal thickening, disruption of the internal elastic lamina, chronic inflammatory infiltration with giant cells. Pathological confirmation requires destruction of the internal elastic lamina and inflammatory cell infiltration (acute phase) or fibrosis (chronic phase). Giant cells are not essential for definitive diagnosis.
False negatives: False negative rate of 3–5% due to skip lesions. Some reports indicate up to 61% 6). GCA cannot be ruled out even with negative TAB.
Timing: Biopsy should be performed within a few days after starting steroid therapy.
Imaging Studies
Temporal artery ultrasound (CDUS): Non-invasive and repeatable. Sensitivity 77%, specificity 96% 4). Characteristic findings include halo sign (hypoechoic ring due to vessel wall thickening), compression sign, stenosis, and occlusion. Due to skip lesions, comprehensive bilateral and multi-region examination is important 4). When halo sign is positive bilaterally, specificity increases to 100% 4).
PET-CT: Can detect abnormal uptake in the aorta and its branches in large-vessel GCA (LV-GCA). In the GAPS study, sensitivity 92%, specificity 85% 6).
MRI: Useful for differentiating AAION from NAION. Evaluate contrast enhancement of the optic nerve sheath and orbital fat (central bright spot).
Ophthalmic Examinations
Fluorescein angiography (FA): Delayed filling of the optic disc and delayed filling or defects (segmental ischemia) of the peripapillary choroid are characteristic of AAION. These may be observed even before the appearance of disc edema. This is an important distinguishing feature from NAION.
OCT/OCTA: Useful for evaluating segmental disc edema, retinal nerve fiber layer (RNFL) thickness, and the ischemic status of the optic disc.
ACR Classification Criteria (1990) and 2022 ACR/EULAR Classification Criteria
Giant cell arteritis must be differentiated from other vasculitides such as polyarteritis nodosa, granulomatosis with polyangiitis (Wegener), and SLE. An important distinguishing feature is that GCA does not affect the lungs or kidneys. Ocular syphilis can present with symptoms similar to GCA 10). Occult GCA without systemic symptoms (about 20%) should also be considered.
QCan giant cell arteritis be ruled out even if temporal artery biopsy is negative?
A
No, it cannot be ruled out. The false-negative rate due to skip lesions (inflammation present only in a portion of the vessel) is 3–5% (some reports indicate up to 61% 6)). Even if TAB is negative, treatment should be continued if clinical suspicion of GCA is high with elevated ESR and CRP. It is important to comprehensively evaluate clinical findings, blood tests, and ultrasound findings.
When visual impairment is suspected, treatment should be started immediately without waiting for a confirmatory biopsy. The main goal of treatment is prevention of involvement in the fellow eye, and improvement of vision in the affected eye is rarely expected. Vision improves with treatment in only 15–20% of cases. Inpatient high-dose steroid intravenous therapy is preferred.
Consider when side effects from long-term steroid use (Cushingoid syndrome, hyperglycemia, osteoporosis, gastrointestinal symptoms, etc., occurring in about 60% of patients) become problematic.
Tocilizumab (IL-6 receptor inhibitor): Approved by the FDA in 2017 for the treatment of GCA. Randomized controlled trials (RCTs) have demonstrated its glucocorticoid-sparing effect and efficacy in achieving remission over 12 months 4). It has been reported effective in steroid-resistant AAION. Use of TCZ 162 mg subcutaneously has also been reported in GCA cases after COVID-19 vaccination 8)9).
Methotrexate: Increases the rate of sustained glucocorticoid discontinuation and reduces the risk of relapse. In case reports, a dose of 15 mg/week has been used in combination 1). In case of relapse, increasing glucocorticoid dose plus adding MTX may be recommended.
Low-dose aspirin: May be considered for prevention of cardiac and cerebrovascular ischemic complications.
QDoes vision improve with glucocorticoid treatment?
A
Improvement of vision in the affected eye is rarely expected. Vision improves in only about 15–20% of cases, and most patients have residual vision loss. The main goal of glucocorticoid treatment is to prevent involvement of the fellow eye.
The pathogenesis of giant cell arteritis involves two major immune response mechanisms. It is a T-cell-mediated granulomatous vasculitis initiated by activation of dendritic cells in the vessel wall, selectively affecting medium to large arteries.
Blood supply to the optic nerve is mainly provided by the SPCA and branches of the central retinal artery.
The SPCA supplies the prelaminar and laminar regions and also contributes to the peripapillary choroidal circulation.
In GCA, thrombotic occlusion of the SPCA (particularly affected in 20% of cases) causes optic disc ischemia.
Postmortem examination of acute AAION shows optic disc edema with necrosis of the prelaminar, laminar, and retrolaminar regions, along with chronic inflammatory cell infiltration.
Fragmentation of the internal elastic lamina is characteristic, and giant cells are located near the fragmented internal elastic lamina. In the acute phase, lymphocytic infiltration is predominant, and fibrosis occurs in the chronic phase. As a healing response to inflammation, intimal thickening, myofibroblast proliferation, and extracellular matrix deposition occur, leading to vascular stenosis and occlusion.
7. Latest Research and Future Perspectives (Investigational Reports)
Upadacitinib, an oral JAK1-selective inhibitor, received FDA approval for the treatment of GCA in 2025. It is attracting attention as a novel therapeutic option targeting the IL-6–JAK–STAT pathway.
Tocilizumab has demonstrated a glucocorticoid-sparing effect and efficacy in achieving remission over 12 months in RCTs 4), and is becoming established as an alternative therapy to reduce the toxicity associated with long-term glucocorticoid use.
A rapid diagnostic pathway for giant cell arteritis using ultrasound is becoming widespread in Europe. The introduction of a fast-track pathway has been shown to reduce vision loss, limit overtreatment, and improve cost-effectiveness 4). Ultrasound is non-invasive, repeatable, and can evaluate multiple arterial territories at once, positioning it as a key tool for early diagnosis.
A subtype of GCA arising in the context of myelodysplastic syndrome (MDS) (GCA-MDS) has been recognized. Autoimmune diseases are reported to occur in 10–20% of MDS patients. GCA-MDS may have a lower prevalence of classic symptoms (headache, jaw claudication, AAION, etc.) than typical GCA, tends to become steroid-dependent, and has lower steroid-free survival and relapse-free survival rates. Addition of hypomethylating agents (azacitidine/decitabine) may be beneficial, and a prospective study (NCT02985190) is ongoing. The largest reported series is 21 cases from a French multicenter study in 2019.
A report indicates a 70% increase in GCA incidence during the COVID-19 pandemic 2). Multiple reports suggest an increase in GCA cases in 2020, with a rise in ocular complication rates and possible involvement of endothelial damage, Th1 immunity, and monocyte-macrophage lineage 2). There are also case reports suggesting that SARS-CoV-2 may have triggered GCA.
Multiple cases of GCA onset after COVID-19 vaccination have been reported. Yoshimoto et al. (2023) reviewed 14 cases and reported that the time from onset to diagnosis ranged from 2 weeks to 4 months (mean approximately 6 weeks) 8). Blindness occurred in 2 of the 14 cases.
Sverdlichenko et al. (2022) reported Horner syndrome (partial ptosis and miosis) in 2 of 53 GCA patients 5). The presumed mechanism is ischemia of the first-order sympathetic neurons in the brainstem due to vasculitis of the vertebral artery and its branches. For new-onset Horner syndrome in patients aged 50 years or older, checking for GCA symptoms and inflammatory markers is recommended.
Hayreh et al. (2021) reported a case of giant cell arteritis in 3 of 5 siblings of Indian descent, suggesting an autosomal recessive inheritance pattern 7). This is noted as the first report of familial GCA in non-White individuals.
Szydełko-Paśko U, Przeździecka-Dołyk J, Kręcicka J, Małecki R, Misiuk-Hojło M, Turno-Kręcicka A. Arteritic Anterior Ischemic Optic Neuropathy in the Course of Giant Cell Arteritis After COVID-19. The American journal of case reports. 2022;23:e933471. doi:10.12659/AJCR.933471. PMID:35015754; PMCID:PMC8762612.
Jalaledin DS, Ross C, Makhzoum JP. Rare Ischemic Complications of Giant Cell Arteritis: Case Series and Literature Review. The American journal of case reports. 2022;23:e937565. doi:10.12659/AJCR.937565. PMID:36240129; PMCID:PMC9578098.
Piccus R, Hansen MS, Hamann S, Mollan SP. An update on the clinical approach to giant cell arteritis. Clinical medicine (London, England). 2022;22(2):107-111. doi:10.7861/clinmed.2022-0041. PMID:35304369; PMCID:PMC8966809.
Sverdlichenko I, Lam C, Donaldson L, Margolin E. Horner Syndrome in Giant Cell Arteritis: Case Series and Review of the Literature. Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society. 2022;42(3):340-345. doi:10.1097/WNO.0000000000001593. PMID:35427255.
Stewart C, Asif RH, Dakkak T, Singh H, Javaid MA, Patel N. Diagnostic Dilemmas in Giant Cell Arteritis: Overcoming Anchoring Bias. Case reports in rheumatology. 2025;2025:6632374. doi:10.1155/crrh/6632374. PMID:40726518; PMCID:PMC12303627.
Yoshimoto K, Kaneda S, Asada M, Taguchi H, Kawashima H, Yoneima R, Matsuoka H, Tsushima E, et al. Giant Cell Arteritis after COVID-19 Vaccination with Long-Term Follow-Up: A Case Report and Review of the Literature. Medicina (Kaunas, Lithuania). 2023;59(12). doi:10.3390/medicina59122127. PMID:38138230; PMCID:PMC10744572.
Wakabayashi H, Iwayanagi M, Sakai D, et al. Development of giant cell arteritis after vaccination against SARS-CoV2. Medicine. 2023;102(21):e33814.
Qadir A, Khakwani AS, Khan MR, et al. Ocular Syphilis Mimicking Giant Cell Arteritis. Cureus. 2022;14(9):e29286.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.