Sebaceous carcinoma (sebaceous carcinoma, SGC) is a rare, highly malignant tumor that arises from the sebaceous glands of the eyelid—the meibomian glands, glands of Zeis, sebaceous glands of the lacrimal caruncle, and sebaceous glands of the eyebrow skin. It is one of the most important malignant tumors of the eyelid, and most cases originate from the meibomian glands. Because there are about 50 meibomian glands in the upper eyelid and about 25 in the lower eyelid, it occurs more often in the upper eyelid.
The disease is positioned very differently in Europe and North America compared with East Asia. Among all malignant eyelid tumors, basal cell carcinoma accounts for 80-95% in Europe and North America, while sebaceous carcinoma accounts for only 1-3%1). By contrast, the proportion of sebaceous carcinoma is much higher in Asian populations.
The epidemiologic differences between Asia and Europe and North America are shown below.
However, the higher proportion of sebaceous carcinoma in Asians is because the proportion of basal cell carcinoma is relatively lower, whereas the incidence of sebaceous carcinoma itself is higher in White people (2.03 vs Asian/Pacific Islander 1.07 per million)1). In Asians with an eyelid malignant tumor, the chance that it is sebaceous carcinoma is 6.21 times that in non-Asians (range 3.8-10.1)1). In Japan, it is the second most common among eyelid malignant tumors after basal cell carcinoma.
Onset is mainly after the 50s, and the mean age has been reported as 57-72 years, with 58 years in Indians1). In 25% of cases, it can also occur in the head and neck, other skin, and the genital organs besides the eyelid.
Muir-Torre syndrome: An autosomal dominant inherited disorder in which sebaceous tumors and visceral malignancies (gastrointestinal, endometrial, urinary tract) occur together. It is associated with mutations in DNA mismatch repair genes (MLH1, MSH2, MSH6), and sebaceous carcinoma develops in 24% of patients with Muir-Torre syndrome. Sebaceous carcinoma in Muir-Torre syndrome is considered less invasive than sporadic cases.
QIf an eyelid mass is diagnosed as sebaceous carcinoma, should we suspect other cancers as well?
A
Muir-Torre syndrome should be considered. It is an inherited disorder in which sebaceous tumors and visceral malignancies such as colorectal cancer occur together, and if loss of expression is seen on immunostaining for MLH1, MSH2, or MSH6, referral to gastroenterology or a similar department is recommended.
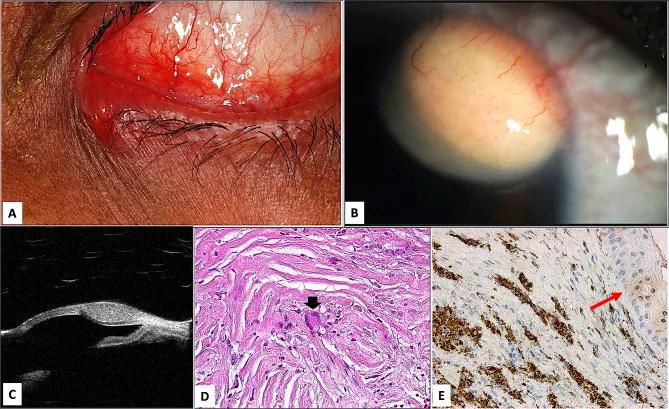
Nodular lesion with ulceration on the lower eyelid
Alkatan HM, et al. Clinicopathological study of ophthalmic cutaneous and mucocutaneous non-langerhans cell histiocytic lesions. BMC Ophthalmol. 2024. Figure 3. PMCID: PMC10949701. License: CC BY.
A is a nodular lesion of adult xanthogranuloma (AXG) with central ulceration, seen on the right lower eyelid of a man clinically diagnosed with sebaceous carcinoma. It corresponds to the eyelid nodule discussed in the section “2. Main symptoms and clinical findings”.
Yellowish nodular mass: A yellow appearance caused by lipid inside the tumor cells is characteristic. It often arises at the upper eyelid margin and has an irregular surface with tumor vessels that bleed easily.
Observation by eyelid eversion: It is important to turn the eyelid over and also check the conjunctival side.
Diffuse type (7%)
Intraepithelial spread without a mass: A type that spreads thinly from the meibomian gland opening to the eyelid margin skin and palpebral conjunctiva.
Eyelash loss (madarosis): One of the characteristic findings of the diffuse type. Diagnosis is often most delayed.
The tumor site in sebaceous carcinoma is the upper eyelid in 59%, the lower eyelid in 29%, the inner canthus in 3%, and the outer canthus in 2%1).
Pagetoid spread: A characteristic pattern in which tumor cells spread in sheets within the epithelium of the palpebral and bulbar conjunctiva away from the main lesion. It can show firework-like tumor vessels and tumor cell proliferation covering the entire palpebral conjunctiva, and may form skip lesions.
QWhy is sebaceous carcinoma called the great masquerader?
A
Because it closely resembles several conditions, such as chalazion, blepharitis, and basal cell carcinoma, making clinical diagnosis extremely difficult. Of all eyelid tumors, sebaceous carcinoma is said to account for 0.5%, but only 1 of 29 cases (in a Canadian study) was correctly diagnosed clinically. Recurrent chalazia that are repeatedly incised and drained should always raise suspicion for sebaceous carcinoma.
Older age: Median age at onset is 57 to 72 years. Aging is the main risk factor.
Sex difference: Periocular sebaceous carcinoma is slightly more common in women (male-to-female ratio 1:1.5)1).
Upper eyelid predominance: because there are more meibomian glands (about 50 in the upper eyelid vs about 25 in the lower eyelid).
History of periocular radiotherapy: This can also be a risk factor even in younger people.
Immunosuppression: Immunosuppressed states, such as after solid organ transplantation or with lymphoma, may also be associated.
Muir-Torre syndrome: Mutations in DNA mismatch repair genes (MLH1, MSH2, MSH6).
Tumor size: When it exceeds 15 mm, the risk of regional lymph node metastasis increases.
QIs it true that sebaceous carcinoma is more common in Asians?
A
In Asians with an eyelid malignancy, the chance that it is sebaceous carcinoma is 6.21 times higher than in non-Asians1). However, this refers to the relative proportion; the incidence of sebaceous carcinoma itself (per population) is actually higher in White people (2.03 per million) than in Asian/Pacific Islander people (1.07 per million). Because basal cell carcinoma is less common in Asians, sebaceous carcinoma appears relatively more common.
Maintaining a high index of suspicion is most important. Actively suspect sebaceous carcinoma in the following cases.
Atypical or recurrent chalazion (repeated recurrence after incision)
Chronic blepharitis and persistent blepharoconjunctivitis that do not respond to treatment
Yellowish thickening of the eyelid or a yellow mass
Eyelid lesions with eyelash loss
Even if it appears to be a chalazion, the curettage material should always be submitted for pathological examination. In some cases, improvement with antibiotic eye ointment can help distinguish Paget-like spread from eyelid margin inflammation.
Excisional biopsy of the primary lesion: Perform a wide excisional biopsy, mark the margins, and submit it to pathology.
Conjunctival mapping biopsy: To determine the extent of the lesion, take biopsies from multiple sites in the palpebral and bulbar conjunctiva of all four quadrants in both eyes. This is essential for defining the extent of Paget-like spread.
Well-differentiated cases: Lobular arrangement, with cytoplasmic vacuolization in the center.
Mixture of sebaceous cells and undifferentiated basaloid cells: Nuclear pleomorphism, high mitotic activity.
Traditional fat stains (Oil Red O, Sudan IV): Fresh frozen tissue is required, so practicality is limited. They are now replaced by immunohistochemistry.
The current standard immunohistochemical markers are shown below.
Marker
Features
Adipophilin
Intracellular lipid droplet-associated protein. Highly sensitive and practical for sebaceous differentiation3)
Androgen receptor
Usually positive in eyelid sebaceous carcinoma
Epithelial membrane antigen (EMA)
Positive
Muir-Torre syndrome screening: Check for loss of expression by immunohistochemical staining for MLH1, MSH2, and MSH6.
Differentiation from sebaceous carcinoma: glycogen is positive on periodic acid-Schiff (PAS) stain (sebaceous carcinoma contains lipids and is negative on PAS stain)
QWhen should Muir-Torre syndrome be suspected?
A
Muir-Torre syndrome should be suspected when sebaceous tumors (such as sebaceous carcinoma or sebaceous adenoma) are found together with an internal malignancy, especially colorectal cancer. If loss of expression is confirmed on pathology specimens by immunostaining for MLH1, MSH2, and MSH6, referral for further evaluation to departments such as gastroenterology and gynecology is recommended.
Intraoperative margin assessment with frozen sections is desirable.
If the tarsal defect is one-third or less, reconstruction can be done with simple closure or a local flap.
There is also a method of reconstructing the anterior lamella (skin and orbicularis oculi muscle) and posterior lamella (tarsus and conjunctiva) separately.
For posterior lamellar reconstruction, autologous tissue such as hard palate with mucosa, septal cartilage, auricular cartilage + labial mucosa is used.
Mohs micrographic surgery or complete circumferential peripheral and deep margin assessment (CCPDMA): first-line treatment in Europe and the United States. This method evaluates all tissue in horizontal sections while removing it, checking for tumor cells at the margins.
Indian treatment protocol (reference): For T1–T3 tumors, wide excision with a 4 mm margin + frozen-section control -> eyelid reconstruction. For T4 tumors, consider preoperative chemotherapy (5-fluorouracil + cisplatin/carboplatin every 3 weeks) or orbital exenteration2).
It is performed for cases with orbital invasion, large and deeply infiltrating lesions, and extensive bulbar conjunctival spread. The reported AJCC stage-specific rates of use are T1 3%, T2 3%, T3 8%, and T4 63%2).
External beam radiation therapy to the orbit is given for microscopic residual tumor after orbital exenteration2).
Radiation therapy (55–66 Gy) is considered effective for local control, but the optimal dose has not been established.
In Hata (2012), 13 cases showed a 5-year local recurrence-free rate of 100%4).
If regional lymph node metastasis occurs, neck dissection plus postoperative chemotherapy and radiation therapy are performed2).
QHow wide a safety margin is needed for surgery for sebaceous carcinoma?
A
In Japan, excision with a safety margin of at least 3 mm is standard. In Western countries, Mohs micrographic surgery or complete circumferential peripheral and deep margin assessment is the first choice, and the tissue is removed while evaluating all margins. For T4 tumors and cases with orbital invasion, orbital exenteration is considered.
Sebaceous carcinoma is a malignant tumor arising from the glandular epithelium of the sebaceous glands. Reported sites of origin are 92% from the meibomian glands, 6% from the glands of Zeis, and 2% from the lacrimal caruncle2).
Histologically, sebaceous cells (cells with vacuolated cytoplasm rich in lipids) and undifferentiated basaloid cells are mixed, and the degree of differentiation ranges from well differentiated to poorly differentiated. The lipids within the tumor cells give the lesion a yellow appearance on gross examination.
Mechanism of pagetoid spread: A pattern in which malignant cells individually migrate and proliferate in epithelium away from the main tumor—palpebral conjunctiva, bulbar conjunctiva, and skin. It forms skip lesions, and tumor cells may be present in areas that appear free of disease on gross examination. For this reason, grasping the extent with conjunctival mapping biopsy is essential for treatment.
Molecular mechanism of Muir-Torre syndrome: An autosomal dominant inherited disorder caused by mutations in DNA mismatch repair genes (MLH1, MSH2, MSH6, PMS2). These mutations abolish the ability to repair DNA replication errors, and sebaceous tumors arise as mutations accumulate in tumor suppressor genes.
7. Latest research and future prospects (research-stage reports)
Morawala (2023) examined the AJCC 8th edition T classification in 119 cases of sebaceous carcinoma and showed that T classification is useful for predicting prognosis2). For T4 tumors, the hazard ratios were 2.38 for lymph node metastasis, 4.30 for distant metastasis, and 6.62 for metastasis-related death. In addition, the 8th edition changed the definition of T1 from 5 mm or less in the 7th edition to 10 mm or less, confirming that downstaging occurs.
Li & Finger (2021) reported that for T2bN0M0 orbital sebaceous carcinoma, a total of 56 Gy was delivered after resection + cryotherapy + ultrathick amniotic membrane transplantation, using high-dose-rate brachytherapy (2,000 cGy/5 fractions) plus electron beam external beam radiotherapy (36 Gy/20 fractions)5). One year later, visual acuity was 20/20, with no radiation retinopathy or optic neuropathy. However, cervical lymph node metastasis occurred.
Radiation therapy with hydrogen peroxide–impregnated gauze
Adachi (2022) performed electron beam therapy of 60 Gy/30 fr plus hydrogen peroxide–impregnated gauze for a 97-year-old patient with unresectable preauricular sebaceous carcinoma4). Eight months later, the patient achieved a gross complete response. The only adverse event was Grade 2 radiation dermatitis. A radiosensitizing effect of hydrogen peroxide was suggested, but this was a report of a small number of cases and requires further validation.
Kaliki S, Bothra N, Bejjanki KM, Nayak A, Ramappa G, Mohamed A, et al. Malignant Eyelid Tumors in India: A Study of 536 Asian Indian Patients. Ocular oncology and pathology. 2019;5(3):210-219. doi:10.1159/000491549. PMID:31049330; PMCID:PMC6489076.
Morawala A, Mohamed A, Krishnamurthy A, Jajapuram SD, Kaliki S. Sebaceous gland carcinoma: analysis based on the 8(th) edition of American Joint Cancer Committee classification. Eye (Lond). 2023;37(4):714-719. doi:10.1038/s41433-022-02025-2. PMID:35347292; PMCID:PMC9998849.
Ramachandran V, Tumyan G, Loya A, Treat K, Vrcek I. Sebaceous Carcinoma Masquerading As Orbital Cellulitis. Cureus. 2022;14(2):e22288. doi:10.7759/cureus.22288. PMID:35350510; PMCID:PMC8933264.
Adachi A, Oike T, Tamura M, Ota N, Ohno T. Radiotherapy With Hydrogen Peroxide-Soaked Gauze for Preauricular Sebaceous Carcinoma. Cureus. 2022;14(7):e27464. doi:10.7759/cureus.27464. PMID:35923494; PMCID:PMC9339371.
Li F, Stewart RD, Finger PT. Interstitial Brachytherapy for Orbital Sebaceous Carcinoma. Ophthalmic plastic and reconstructive surgery. 2021;37(6):e215-e217. doi:10.1097/IOP.0000000000002031. PMID:34314398; PMCID:PMC8565506.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.