Eyelid squamous cell carcinoma is an invasive malignant tumor that arises from the stratum spinosum of the skin epithelium. It is the second most common eyelid malignancy after basal cell carcinoma and accounts for less than 5% of all eyelid malignant neoplasms.
Incidence has been reported as 0.09 to 2.42 per 100,000 population, and in the United States and Canada the age-adjusted incidence of squamous cell carcinoma has increased by 50% to 200% over the past several decades. The average age at diagnosis is generally around 60 years.
Regional differences: In Europe and the United States, basal cell carcinoma accounts for most eyelid malignancies (80% to 95%), while squamous cell carcinoma accounts for only 5% to 10%. In a study of 536 cases in India, squamous cell carcinoma accounted for 18%, ranking third after sebaceous carcinoma (53%) and basal cell carcinoma (24%)1). A Japanese study also reported that squamous cell carcinoma accounted for 48% of eyelid malignant tumors, indicating a higher proportion in Asia than in Europe and the United States1).
In a retrospective study of 536 cases in India (Kaliki 2019), the mean age at diagnosis of squamous cell carcinoma was 55 years (range 8 to 90), and the male-to-female ratio was 1:1.1, with a slight female predominance1). The most common sites were the upper eyelid at 40% and the lower eyelid at 41%, with no major difference1).
Reported metastasis rates range from 1% to 21%, and it shows more invasive biological behavior than basal cell carcinoma.
QHow often does eyelid squamous cell carcinoma occur?
A
It is estimated at 0.09 to 2.42 per 100,000 population. In Europe and the United States it accounts for 5% to 10% of eyelid malignancies, but in Asia the proportion is higher, and in Japan it has been reported to account for about half of eyelid malignant tumors.
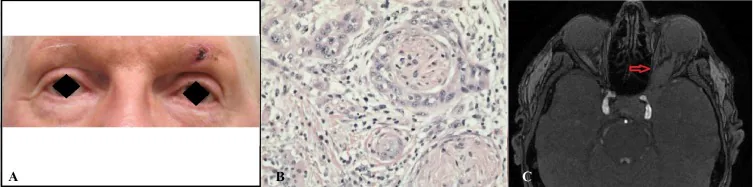
Clinical appearance, histologic findings, and MRI images of squamous cell carcinoma
Spitzer N, et al. Recurrent Squamous Cell Carcinoma of the Eyelid Presenting as Trigeminal Neuralgia. Cureus. 2016. Figure 1. PMCID: PMC5235655. License: CC BY.
Clinical appearance (A), histopathology (B), and MRI image (C) of squamous cell carcinoma (SCC). This corresponds to the eyelid mass discussed in the section “2. Main symptoms and clinical findings.”
The clinical appearance differs greatly between precursor lesions and invasive squamous cell carcinoma.
Precursor lesion
Actinic keratosis: A hyperkeratotic lesion common in fair-skinned people in their 40s and older. It is round to oval and has an erythematous base. It is considered squamous cell carcinoma in situ.
Bowen disease (in situ carcinoma): appears as a persistent brown to red patch. It is often misdiagnosed as psoriasis or eczema. It is strongly associated with HPV type 16.
Cutaneous horn: has a keratin cap on a papule- to nodule-like base. The base may be accompanied by squamous cell carcinoma in situ or invasive squamous cell carcinoma, so removal is always needed.
Keratoacanthoma: a cup-shaped nodule with a central keratin crater. It is sometimes classified as a subtype of squamous cell carcinoma.
Invasive squamous cell carcinoma
Nodular type: hyperkeratotic nodule with crusting or fissures (52% in the Kaliki study).
Ulcerative type: red base with well-defined, firm, everted edges (40% in the Kaliki study).
Eyelid findings: lash loss, telangiectasia, distortion of eyelid structure, and eyelid malposition.
It is very rare for it to start on the palpebral conjunctival surface. When keratinization is marked, it appears white; when tumor vessels are present, it appears as a flat red lesion.
The development of squamous cell carcinoma is promoted by multiple overlapping risk factors.
Ultraviolet exposure: the most important modifiable risk factor. Cumulative UVA and UVB exposure damages DNA directly (base substitutions) or indirectly (reactive oxygen species)2)
Aging: Risk increases with age
Fair skin (low Fitzpatrick skin type): Risk is higher in people with fair skin2)
Immunosuppression: After organ transplantation, use of immunosuppressive drugs, and HIV infection increase the risk2)
Human papillomavirus (HPV) infection: In Bowen disease, the link with HPV type 16 is strong
Xeroderma pigmentosum: Due to autosomal recessive mutations in DNA repair genes (XPA–XPF), the risk of non-melanoma skin cancer is 10,000 times higher than in the general population2)
Precancerous lesions: It progresses step by step from actinic keratosis → squamous cell carcinoma in situ → invasive squamous cell carcinoma → metastatic squamous cell carcinoma
Other: exposure to petroleum derivatives and arsenic, smoking, albinism, old burn scars (Marjolin ulcer), chronic ulcers
QDoes the risk of eyelid squamous cell carcinoma increase after organ transplantation?
A
Yes, it increases greatly. Cutaneous squamous cell carcinoma is one of the most common malignancies after solid organ transplantation, and the incidence within 5 years reaches 30% after lung transplantation and up to 26% after heart transplantation. Regular skin and eye examinations are important after transplantation.
The agreement rate between clinical and pathological diagnoses is low in squamous cell carcinoma, at 46% (compared with 86% for basal cell carcinoma and 91% for sebaceous carcinoma), so a definitive diagnosis by biopsy is essential1). During the examination, assess the following.
Document the lesion’s general appearance, size, ulceration, eyelash loss, and telangiectasia
Perform a complete ophthalmic examination, including eye movements and proptosis
Examine the entire face and sun-exposed areas, and check facial sensation
Palpate the regional lymph nodes (preauricular, sublingual, submandibular, and cervical)
Observe the eyelids during opening and closing, and inspect the conjunctival surfaces of the upper and lower eyelids
For large tumors, use orbital CT/MRI to check the internal structure and whether the tumor has spread into the orbit
Complete surgical excision with histologic confirmation of tumor-free margins is the standard treatment with the strongest evidence. Squamous cell carcinoma may have less distinct borders than basal cell carcinoma, making it difficult to define the clinical tumor margin.
Mohs micrographic surgery: A technique in which the excision margin is examined pathologically in real time during removal. It allows reliable excision while minimizing tumor tissue
Excision with intraoperative frozen-section pathology: Intraoperative confirmation of the resection margin
Early lesion (limited to the palpebral conjunctival surface): Complete excision including part of the tarsal plate. After confirming negative margins, add 2–3 cycles of cryocoagulation (freeze-thaw) to the excision surface
When performing wide full-thickness eyelid excision: Reconstruction using a switch flap or the Cutler-Beard procedure
Orbital exenteration: Performed when there is orbital invasion and poor visual prognosis, if the cavernous sinus has not been reached. It was performed in 19% of squamous cell carcinoma cases1)
In Kaliki 2019, wide excision biopsy was performed in 82% of all eyelid malignant tumors (76% in squamous cell carcinoma)1).
Tissue destruction using liquid nitrogen. It is indicated only for actinic keratosis and squamous cell carcinoma in situ. It is not suitable for invasive cancer. A 5-year survival rate of 95% has been reported for superficial, early squamous cell carcinoma in situ.
It is used as monotherapy for patients whose surgical risk is too high, or as postoperative adjuvant therapy for cancers with perineural or lymph node spread or unclear margins. Irradiation is given 3 to 5 times per week for about 1 to 2 months.
Imiquimod ointment: An immunomodulator. Indicated for actinic keratosis, Bowen disease (precancerous lesion), and superficial squamous cell carcinoma. Apply 3 times a week for 4 to 6 weeks
Mitomycin C eye drops (0.04%): Indicated when conjunctival lesions, such as pagetoid spread, are confined to the epithelium. Instill 4 times a day, 1 week on and 1 week off, repeated for 2 to 3 cycles
5-fluorouracil eye drops (1%): Likewise indicated for lesions confined to the epithelium. Instill 4 times a day, 2 to 4 days on and 1 month off, repeated for 2 to 6 cycles
The treatment outcomes in 99 patients with squamous cell carcinoma in India are shown below1).
Indicator
Rate
Tumor recurrence
8%
Regional lymph node metastasis
8%
Regional lymph node metastasis
4%
Disease-related death
4%
Eye preservation
79%
At the 5-year Kaplan-Meier estimate, regional lymph node metastasis was 22%, distant metastasis 11%, and metastasis-related death 11%1).
QWhat is the risk of recurrence after surgery for eyelid squamous cell carcinoma?
A
In the Kaliki 2019 study, postoperative tumor recurrence was seen in 8%. The 5-year Kaplan-Meier estimate showed regional lymph node metastasis reaching 22%, so regular follow-up after surgery is important.
Ultraviolet light directly damages DNA (base substitution) or indirectly damages it (oxidative damage via reactive oxygen species)2). Sunburn-induced apoptosis acts as a defense mechanism, but if DNA repair cannot keep up, mutations accumulate.
p53 inactivation: The p53 tumor suppressor is directly damaged and inactivated by ultraviolet exposure. Its functions in cell-cycle arrest and apoptosis regulation are lost, allowing mutated cells to proliferate2)
Genomic instability: The genomic instability of keratinocytes is likely due to p53 inactivation
Proliferation and hyperkeratosis → mild to moderate dysplasia → severe dysplasia and carcinoma in situ → invasive squamous cell carcinoma → metastatic squamous cell carcinoma
Marjolin ulcer: A condition in which SCC develops from scar tissue in chronic nonhealing wounds or long-standing burn scars.
The stage distribution in Kaliki 2019 was T1: 26%, T2: 37%, T3: 7%, T4: 29%1). Histologic grade ranges from G1 (well differentiated) to G4 (undifferentiated), and a lower grade is associated with a better prognosis.
7. Latest Research and Future Outlook (Reports at the Research Stage)
Ye et al. (NEJM 2025) reported a case of treatment-resistant invasive cutaneous squamous cell carcinoma with genome integration of β-HPV19 in a 34-year-old woman who had impaired T-cell receptor signaling due to a germline ZAP70 mutation3). In this case, no typical squamous cell carcinoma driver mutations (TP53, NOTCH1/2, CDKN2A) were detected, and the ultraviolet mutational signature was also low at 26% (compared with the average of 77% in ordinary cutaneous squamous cell carcinoma). After allogeneic hematopoietic stem cell transplantation restored T-cell receptor signaling, the HPV-specific T-cell response recovered, and over 35 months of follow-up all HPV-related disease, including cutaneous squamous cell carcinoma, regressed stably.
This report suggests that adaptive immune T-cell responses are involved in controlling the development and progression of squamous cell carcinoma3).
Semiplimab (an anti-PD-1 antibody) is FDA-approved for unresectable and metastatic cutaneous squamous cell carcinoma, and further expansion of its indications is expected in cases that spread to the orbit or lymph nodes. As the role of immune surveillance becomes clearer, the increased risk of squamous cell carcinoma in immunosuppressed states (after organ transplantation, hematologic malignancies, etc.) is also thought to be related to abnormal control of T-cell responses2)3).
QIs immunotherapy effective for eyelid squamous cell carcinoma?
A
The anti-PD-1 antibody semiplimab is FDA-approved for unresectable and metastatic cutaneous squamous cell carcinoma. In addition, there are case reports of tumor regression after immune reconstitution with hematopoietic stem cell transplantation in HPV-driven squamous cell carcinoma. However, the latter is research-stage knowledge and is not a standard treatment.
Early detection and complete removal generally lead to a good prognosis. However, it shows more aggressive biological behavior than basal cell carcinoma and carries a risk of spread to the orbit, lymph nodes, and distant organs. Cases with malignant orbital invasion should be managed in collaboration with multiple specialties, such as medical oncology and radiation oncology.
Key points for follow-up are as follows.
Regular postoperative eye examinations and palpation of the regional lymph nodes
Regular observation of the skin, including sun-exposed areas of the entire face
Lifestyle guidance on sunscreen use, reducing sun exposure, and avoiding alcohol and smoking
More frequent follow-up in patients with immunosuppression
The 5-year Kaplan-Meier estimate showed 22% local lymph node metastasis, 11% distant metastasis, and 11% metastasis-related death1), indicating the need for long-term surveillance.
Kaliki S, Bothra N, Bejjanki KM, Nayak A, Ramappa G, Mohamed A, et al. Malignant Eyelid Tumors in India: A Study of 536 Asian Indian Patients. Ocular oncology and pathology. 2019;5(3):210-219. doi:10.1159/000491549. PMID:31049330; PMCID:PMC6489076.
Ye P, Bergerson JRE, Brownell I, Starrett GJ, Abraham RS, Anderson MV, et al. Resolution of Squamous-Cell Carcinoma by Restoring T-Cell Receptor Signaling. The New England journal of medicine. 2025;393(5):469-478. doi:10.1056/NEJMoa2502114. PMID:40742260; PMCID:PMC12370287.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.