Retinal capillary hemangioma is an orange benign tumor that occurs in the retina or optic disc of young individuals. Because it is pathologically similar to cerebellar hemangioblastoma, it is also called retinal hemangioblastoma in recent years. It can be solitary/multiple, unilateral/bilateral, sporadic/syndromic.
When only retinal hemangioblastoma occurs sporadically, it is called von Hippel disease. When accompanied by systemic tumor syndrome, it is diagnosed as VHL disease (von Hippel-Lindau disease). The Japanese Ophthalmological Society glossary uses “retinal hemangioma” in accordance with the VHL Clinical Practice Guidelines (2024 edition), but this article uses the common term “retinal capillary hemangioma.”
VHL disease is an autosomal dominant hereditary tumor syndrome caused by mutations in the VHL gene (3p25-26), a tumor suppressor gene. The frequency is 1 in 36,000 people. In VHL disease, in addition to retinal hemangioma, there are complications in multiple organs including hemangioblastoma of the cerebellum, medulla oblongata, pons, and spinal cord; renal cell carcinoma; pheochromocytoma; and cysts in abdominal organs (pancreas, kidney, adrenal gland). Life prognosis also depends on management of systemic lesions, so multidisciplinary collaboration is essential.
QWhen is VHL disease suspected?
A
According to the diagnostic criteria in the VHL Clinical Practice Guidelines (2024 edition), if there is a family history, diagnosis is made with one or more lesions such as hemangioblastoma or retinal hemangioma1). If there is no family history, diagnosis is made with two or more lesions (including hemangioblastoma or retinal hemangioma), or confirmation of VHL gene mutation plus one lesion. Since sporadic retinal hemangioma in young individuals, especially under 10 years old, is often later diagnosed as VHL disease, systemic screening and genetic testing should be actively considered.
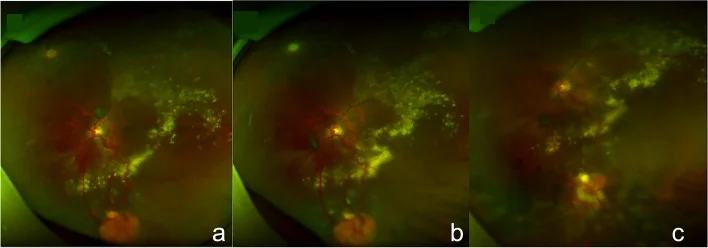
Guo J, Du L, Zhou P, et al. Combined therapy guided by multimodal imaging of fifteen retinal capillary hemangioblastomas in a monocular Von Hippel- Lindau syndrome case report. BMC Ophthalmol. 2022;22(1):205. Figure 4. PMID: 35524216; PMCID: PMC9074324; DOI: 10.1186/s12886-022-02409-8. License: CC BY.
Fundus photographs showing a typical orange-red retinal capillary hemangioma in the peripheral retina with markedly dilated and tortuous feeding vessels (feeding artery and draining vein), and the course of tumor regression after cryocoagulation. This corresponds to the fundus findings discussed in section “2. Main symptoms and clinical findings.”
Retinal hemangioblastoma is classified as follows based on the pattern of occurrence and location.
Peripheral type
Frequency: The most common typical form.
Fundus findings: Forms an orange-red round mass in the peripheral fundus, accompanied by markedly dilated and tortuous feeding arteries and draining veins.
Fundus findings are characterized by solitary or multiple round retinal tumors. Peripheral lesions are accompanied by dilated and tortuous feeding and draining vessels, and the lesions usually appear by age 30. About half of cases are bilateral, and multiple lesions may occur in various parts of the fundus.
The tumor itself is a hemangioblastoma composed of capillaries and foamy stromal cells, and produces large amounts of VEGF (vascular endothelial growth factor). VEGF causes exudative retinal detachment, leading to decreased vision.
Neovascular glaucoma: End-stage complication, accompanied by elevated intraocular pressure and ocular pain.
Marked conjunctival and episcleral vascular dilation: In extremely advanced cases, reports have described right eye NLP and intraocular pressure of 45 mmHg2).
Wide-angle fundus photography and OCT angiography (OCTA) are useful for evaluating lesions and follow-up 1). OCT can assess tumor morphology, the presence of subretinal fluid, and macular edema.
The frequency of VHL disease is 1 in 36,000 people. The number of VHL patients in Japan is estimated to be 600–1,000. The incidence of retinal hemangioma in VHL patients is 40–70%, and the average age of onset is 25 years 1).
Age distribution: Most common in the 10–40 age group. Onset before age 10 occurs in about 5%.
Bilaterality: About half of cases are bilateral.
Multifocality: Multiple tumors may occur in the same eye.
Risk of VHL progression in sporadic cases: When diagnosed as sporadic, 45% of children under 10 years old are later diagnosed with VHL disease.
The VHL gene follows an autosomal dominant inheritance pattern. A germline mutation (first hit) in one allele of the VHL gene, combined with a somatic second hit, leads to loss of tumor suppressor function (two-hit hypothesis).
As a genetic risk factor, all members of families with a pathogenic VHL gene mutation require surveillance, and genetic testing for VHL should be considered in cases of retinal hemangioma under 40 years of age 1).
Fundus examination typically shows a combination of an orange-red tumor in the periphery with dilated and tortuous feeding and draining vessels. The following tests are used in combination for evaluation.
Wide-field fundus photography: Useful for obtaining an overall view of peripheral lesions.
Fluorescein angiography (FA): Identifies tumors and assesses activity. Early and intense fluorescein leakage is a diagnostic hallmark.
OCT/OCTA: Evaluates tumor morphology, quantifies macular edema and subretinal fluid.
In VHL families, fundus examination should begin immediately after birth (age 0) and continue at least once a year 1). Combining non-mydriatic fundus camera with wide-field fundus photography helps prevent overlooking peripheral lesions.
Because VHL disease can cause multiple lesions in organs other than the retina, regular systemic screening by a multidisciplinary team is essential 1).
Head MRI: Screening for hemangioblastomas in the cerebellum, brainstem, and spinal cord.
Abdominal ultrasound, CT/MRI: Search for renal cell carcinoma, pancreatic, renal, and adrenal cysts.
Pheochromocytoma screening: Measurement of urinary catecholamine metabolites.
The above systemic screening should be continued annually.
VHL gene testing is indicated for sporadic retinal hemangioblastoma cases under 40 years of age, and for patients and their families suspected of having VHL disease 1). It is desirable to perform it in conjunction with genetic counseling.
Choroidal hemangioma: Orange-red lesion, but without systemic complications of VHL disease.
Retinal vasoproliferative tumor: Predilection for the inferior periphery. Differentiate from secondary changes.
QWhere are the fundus findings of retinal hemangioma found?
A
Peripheral type often occurs in the peripheral fundus, so detailed fundus examination under mydriasis is necessary. Early small tumors may appear as capillary aneurysms, and wide-angle fundus photography can help prevent oversight. Optic disc type appears as a mass around the disc, and identification of feeding and draining vessels is often difficult.
Treatment is selected according to the location, size, and degree of exudative changes of the hemangioma. Since hemangiomas become refractory as they enlarge, early detection and treatment are important. Initiating treatment while the lesion is small can improve visual prognosis.
Indications: First-line treatment for the peripheral type. For lesions ≤1 disc diameter, a cure can be expected.
Method: Direct coagulation of the hemangioma is repeated until sufficient effect is achieved. Early photocoagulation is also recommended for small lesions <1 disc diameter1).
PDT/Anti-VEGF therapy: In recent years, case reports of photodynamic therapy (PDT) and anti-VEGF drugs (bevacizumab, ranibizumab, etc.) alone or in combination have accumulated3). They are used for adjunctive suppression of exudative changes, but are not covered by insurance and require case-by-case judgment.
Treatment for the optic disc type has not been established1). Laser photocoagulation carries a high risk of optic nerve and macular damage, and the indication must be determined with particular caution. The following treatments have been reported at the case report level, but none are established as standard therapy.
Intravitreal anti-VEGF injection: Expected to suppress exudative changes, but tumor shrinkage effect is limited.
Even after treatment, recurrence and new lesions are likely to occur, so lifelong follow-up is necessary. After each treatment, fundus examination should be performed within 3 to 6 months to confirm the effect and check for new lesions. In VHL disease, multiple lesions appear at different times, so thorough examination of the entire fundus should not be neglected.
For the life prognosis of VHL disease, management of renal cell carcinoma and central nervous system hemangioblastoma is important. In collaboration with multiple departments such as neurosurgery, urology, and endocrinology, appropriate surveillance and intervention for each organ lesion should be performed.
The VHL gene is a tumor suppressor gene located on chromosome 3p25-26, encoding the pVHL protein, a component of the E3 ubiquitin ligase complex. The main function of the pVHL protein is the ubiquitination and proteasomal degradation of the hypoxia-inducible factor (HIF) alpha subunit.
Under normal conditions, HIFα is recognized by pVHL, ubiquitinated, and rapidly degraded. When the VHL gene is inactivated, pVHL function is lost, and HIFα accumulates.
In VHL disease, in addition to a germline mutation (first hit), a second hit in somatic cells (such as loss of heterozygosity, LOH) causes complete loss of VHL gene function, leading to tumor formation.
When HIFα accumulates in the nucleus, transcription of many angiogenesis and cell proliferation-related genes such as VEGF, PDGF, and EPO is constitutively activated. In VHL disease, HIF-2α (EPAS1) functions as a major driver1).
Retinal hemangioblastoma is composed of two types of cells.
Foamy stromal cells: Rich in lipids, they produce large amounts of cytokines including VEGF.
Capillaries: Secondarily induced by VEGF produced by stromal cells.
These stromal cells are the main component of the tumor, and the constant production of VEGF directly causes tumor vascular proliferation and exudative retinal detachment.
Some associations between VHL gene mutation types and clinical phenotypes (e.g., Type 1: non-pheochromocytoma type, Type 2: pheochromocytoma-associated type) are known, but further analysis is needed to clarify the detailed classification and differences in the frequency of ocular involvement.
Belzutifan is a small molecule compound that selectively inhibits HIF-2α. In 2021, the FDA (U.S. Food and Drug Administration) approved it for VHL patients with metastatic renal cell carcinoma, central nervous system hemangioblastoma, and retinal hemangioblastoma 7).
The results for retinal hemangioma in the phase 2 trial (LITESPARK-004) are as follows 1).
Central nervous system hemangioblastoma: Response in 30%.
Major adverse events include anemia (approximately 90%) and fatigue (approximately 66%). Clinical trials in Japan are also planned, and it is attracting attention as a future standard treatment candidate 1).
In a phase 2 trial reported by Jonasch et al. (2021), oral administration of belzutifan 120 mg once daily in patients with VHL disease showed a 100% reduction effect on retinal hemangioblastomas 7).
Photodynamic therapy (PDT) has been reported to be applicable to both peripheral and optic disc types.
di Nicola et al. (2022) reported the efficacy of PDT for retinal hemangioblastomas, particularly showing applicability to juxtapapillary type 4).
Schmidt-Erfurth et al. evaluated the applicability of PDT to optic disc type and the risk of complications 6).
Hussain et al. reported the effect of proton beam therapy for juxtapapillary retinal capillary hemangiomas 5). Case series are accumulating as an option for difficult-to-treat optic disc type.
Although the direct tumor shrinkage effect is limited, there are increasing reports of cases used as adjunctive control of exudative changes 1). The protocol has not been established, and case-by-case judgment is necessary.
QIs belzutifan available in Japan?
A
As of April 2026, belzutifan is not approved for general use in Japan. The FDA approved it in 2021, but in Japan it is in the preparation stage for clinical trials 1). For patients diagnosed with VHL disease for whom standard treatment is difficult, consider consulting with the attending physician or a specialized facility about the possibility of participating in a clinical trial.
QWhat happens if retinal hemangioma is not treated?
A
If the hemangioma enlarges, it becomes refractory and visual prognosis worsens significantly. If exudative retinal detachment extends to the macula, vision loss is likely irreversible, and progression to tractional retinal detachment or neovascular glaucoma can ultimately lead to blindness. In VHL disease, new lesions appear throughout life, so continuous fundus examination is essential alongside treatment.
Lin H, Lin X. Pronounced conjunctival vascular engorgement in von Hippel-Lindau syndrome: a case report. BMC Ophthalmol. 2020 (症例報告).
Krivosic V, Kamami-Levy C, Jacob J, Richard S, Tadayoni R, Gaudric A.. Laser Photocoagulation for Peripheral Retinal Capillary Hemangioblastoma in von Hippel-Lindau Disease. Ophthalmol Retina. 2017;1(1):59-67. doi:10.1016/j.oret.2016.08.004. PMID:31047395.
Di Nicola M, Williams BK Jr, Hua J, Bekerman VP, Mashayekhi A, Shields JA, Shields CL. Photodynamic Therapy for Retinal Hemangioblastoma: Treatment Outcomes of 17 Consecutive Patients. Ophthalmology. Retina. 2022;6(1):80-88. doi:10.1016/j.oret.2021.04.007. PMID:33892136.
Hussain RN, Jmor F, Damato B, et al. Proton beam radiotherapy for retinal capillary haemangioblastoma. Br J Ophthalmol. 2016;100(3):317-321.
Schmidt-Erfurth UM, Kusserow C, Barbazetto IA, Laqua H.. Benefits and complications of photodynamic therapy of papillary capillary hemangiomas. Ophthalmology. 2002;109(7):1256-1266. doi:10.1016/s0161-6420(02)01059-x. PMID:12093647.
Jonasch E, Donskov F, Iliopoulos O, Rathmell WK, Narayan VK, Maughan BL, Oudard S, Else T, Maranchie JK, Welsh SJ, Thamake S, Park EK, Perini RF, Linehan WM, Srinivasan R, MK-6482-004 Investigators.. Belzutifan for Renal Cell Carcinoma in von Hippel-Lindau Disease. N Engl J Med. 2021;385(22):2036-2046. doi:10.1056/nejmoa2103425. PMID:34818478; PMCID:PMC9275515.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.