Macular telangiectasia (MacTel) is a group of diseases characterized by idiopathic telangiectatic capillaries in the macular retina. Capillary dilation and microaneurysms are observed mainly on the temporal side of the fovea, leading to retinal edema or atrophic degeneration in the same area. It was first reported by Gass in 1968 as a distinct entity from Coats disease. 11) Previously called idiopathic macular telangiectasia or idiopathic juxtafoveolar retinal telangiectasis, 12) it is now more simply referred to as MacTel.
The classification by Yannuzzi et al. in 2006 is widely used. 13)
Type 1 (Aneurysmal type)
Laterality: Mostly unilateral
Sex: 90% male
Age of onset: Average around 40 years
Features: Multiple capillary aneurysms and macular edema due to vascular leakage. It lies on the same spectrum as Coats disease and Leber miliary aneurysms.
Type 2 (Perifoveal type)
Laterality: Almost always bilateral
Sex: No sex difference (some reports suggest slightly more common in women)
Age of onset: Average around 55 years
Features: Primarily degeneration of the outer retina. Originates from Müller cell dysfunction, with telangiectasia as a secondary change. Subretinal neovascularization may develop in advanced stages.
Type 3 is a form characterized mainly by vascular occlusion rather than telangiectasia, but it is very rare, and some have proposed excluding it from the classification.
The prevalence is estimated at 0.02–0.10%. 5) According to the MacTel Project report, the mean visual acuity at initial visit was 0.5, with 16% of patients having visual acuity of 1.0 or better, and about half having 0.6 or better. 14) Among type 2 patients, 28% had diabetes and 52% had hypertension. 15) However, the Beaver Dam Eye Study did not confirm a significant association with diabetes or hypertension. 1) In Japan, type 1 is relatively more common, while type 2 is less common than in Western countries. 10)17)
The term “MacTel” usually refers to type 2, so the following discussion focuses on type 2, which is clinically most important.
QWhat are the differences between MacTel types?
A
Type 1 is unilateral with capillary aneurysms and macular edema; type 2 is bilateral with Müller cell degeneration as the core; type 3 is mainly vascular occlusion. Type 2 is the most common and clinically important. For details, see the section “What is Macular Telangiectasia?“.
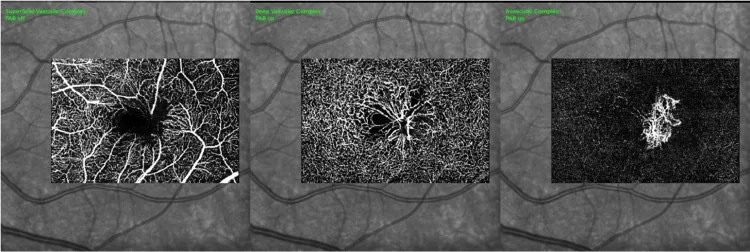
Rao P, et al. Intravitreal Faricimab for the Management of Bilateral Macular Neovascularization Secondary to Macular Telangiectasia Type 2. Cureus. 2025. Figure 3. PMCID: PMC12535685. License: CC BY.
OCT angiography shows irregular foveal avascular zone and right angular vein in the superficial vascular complex of the right eye (A) and left eye (D); vascular invasion and parafoveal telangiectasia in the deep vascular complex of the right eye (B) and left eye (E); and neovascular network with multiple abnormal anastomoses in the avascular complex of the right eye (C) and left eye (F). This corresponds to the telangiectasia discussed in the section “2. Main Symptoms and Clinical Findings.”
In the early stage of type 2 MacTel, subjective symptoms are often minimal. The main symptoms are metamorphopsia, paracentral scotoma, and decreased visual acuity.
Metamorphopsia: The most common complaint. It is noticed as symptoms such as distorted vision of letters.
Paracentral scotoma: Small scotomas occur around the fovea, causing letters to appear missing during reading. This leads to decreased central sensitivity and a marked reduction in reading speed. 10)
Decreased visual acuity: It is noticed when the scotoma extends to the fovea. However, it rarely leads to legal blindness.
Blurred vision and relative scotoma: It may be noticed as slowly progressive binocular symptoms. 10)
In the MacTel Project, the mean visual acuity at initial visit was 0.5, and visual acuity of 0.1 or less was rare. 16) In type 2, when subretinal neovascularization is complicated, rapid visual loss may occur.
Fundus findings in type 2 MacTel are very subtle in the early stage and may be missed by routine fundus examination alone. 5) The proposed 5-stage classification is shown below.
The characteristic fundus findings of type 2 MacTel are as follows.
Decreased retinal transparency: Grayish discoloration of the temporal parafovea. This is the earliest sign.
Telangiectasia: As it progresses, it extends from the temporal side to the entire parafovea10)
Right-angle venules: A characteristic finding in which dilated venules bend at a right angle and run into the deep retinal layers2)
Crystalline deposits: Seen at the vitreoretinal interface of the fovea regardless of disease stage10)
RPE proliferation and pigmentation: Migration and proliferation of RPE are observed within the retina in advanced stages.
Subretinal neovascularization: Occurs in the temporal parafovea during the proliferative stage, accompanied by exudates and hemorrhage1)
In type 1, telangiectasia and microaneurysms are commonly found temporal to the fovea, typically causing macular edema with a ring of hard exudates around the lesion.
QWhat are right-angle venules?
A
Right-angle venules are findings in which dilated venules change direction at a right angle from the superficial to the deep retinal layers. They are characteristic of type 2 MacTel from stage 3 onward and can be traced from the superficial to deep layers on OCT-A.2) They accompany 91.3% of IDZ changes and are important as a precursor to ellipsoid zone loss.
The cause of type 2 MacTel is unknown, but recent research suggests that neurodegeneration is the primary pathology. Advances in imaging such as OCT have led to the belief that Müller cell degeneration is the core of the pathology, and telangiectasia is a secondary change.10)
MacTel 2 is bilateral and suggested to be hereditary. Cases have been reported in monozygotic twins, siblings, and families, with a complex genetic background. 3) Genome-wide association studies (GWAS) have identified three independent genetic loci, two of which are involved in the glycine/serine metabolism pathway. 3) Penetrance and environmental factors also strongly influence the condition, leading to various phenotypic variations. 10)
Metabolomics analyses have reported abnormalities in serine metabolism and sphingolipid metabolism in patients with MacTel 2. 3) Low serine levels are associated with an increase in 1-deoxysphingolipids (1-dSLs), which are neurotoxic lipids. 3) Serine biosynthesis is important for Müller cell oxidative stress defense, and abnormalities in this pathway can lead to macular lesions.
Associations with diabetes, hypertension, obesity, and cardiovascular disease have been suggested, but a causal relationship has not been established. 10) The Beaver Dam Eye Study did not confirm these associations. 1)
OCT is an important and most useful test for diagnosing type 2 MacTel. 10) Early changes include retinal cavities without retinal thickening, retinal thinning due to damage to the outer nuclear layer and photoreceptor layer, and disruption of the temporal ellipsoid zone (EZ). 10) Retinal cavities can form in any retinal layer and, when formed in the fovea, may resemble an outer lamellar hole. 10)
Features of the non-proliferative stage: Retinal thickness does not clearly increase and often decreases. Early loss of the ellipsoid zone (EZ) is observed. Atrophy and cystoid changes in the inner and outer retinal layers that do not correspond to fluorescein leakage on FA. The fact that FA shows little staining further increases the diagnostic value of OCT. 10)
ILM drape: When degeneration extends to the inner retinal layers, only the internal limiting membrane remains, forming a thin “drape.” This is a key diagnostic finding. 5)
Proliferative stage: High-intensity reflection corresponding to subretinal neovascularization appears.
In type 1 OCT, increased retinal thickness and cystoid changes corresponding to FA leakage are seen, which is useful for differentiation from type 2.
Red free images show a ring-shaped or horizontally oval hyperreflective area in the macula. 10) This finding is specific to MacTel type 2 and is useful for diagnosis as it is observed from the early stage. 10) It is more clearly observed with confocal blue light reflectance (CBR). 10)
Non-invasive layer-specific evaluation of retinal vessels is possible, which is useful for diagnosis and follow-up of MacTel. 7)
Telangiectasia of the deep capillary plexus (DCP): The earliest vascular change in MacTel, detected in 100% of cases by OCT-A 2)
Vascular dragging and clustering of the superficial capillary plexus (SCP): Findings of V-shaped displacement toward the fovea
Irregularity of the foveal avascular zone (FAZ): Becomes irregular due to parafoveal vascular changes
Tracking of right-angle vessels: Three-dimensional observation of vessel course from superficial to deep layers is possible 2)
Detection of subretinal neovascularization: Active neovascular networks are visualized in the outer retinal slab 7)
Chandran et al. (2023) reported in a study of 43 eyes that all 36 eyes (100%) with right-angle vessels had DCP telangiectasia, and 89% of them had IDZ changes. Progression occurred stepwise from IDZ attenuation to IDZ loss, followed by EZ attenuation and loss, and the finding of IDZ loss was a predictor of EZ defect (p = 0.002). 2)
It is useful because it can detect functional changes before anatomical changes are recognized. 6)
Decreased macular pigment: An isoreflective image is seen in the parafoveal area. It is present even in the early stage when FA findings are scarce or in asymptomatic periods, and has high diagnostic value. 10)
Foveal hyperautofluorescence: Reflects the loss of lutein pigment (xanthophyll).
Hypoautofluorescent spots in advanced stages: Areas with pigment deposition become hypoautofluorescent due to blockage. 10)
In type 2, dilated capillaries temporal to the fovea show early hyperfluorescence and late leakage. Leakage is mainly from the deep layers rather than the superficial layers. 10) However, leakage is mild, and macular edema is absent or mild. In type 1, more prominent telangiectasia, microaneurysms, and late cystoid macular edema are characteristic.
Differential Diagnosis and Severity Classification
Severity classification: Cases with corrected visual acuity less than 0.3 in the better-seeing eye are classified as severe.10)
QWhat are the differentiating points between type 2 MacTel and diabetic macular edema?
A
In type 2 MacTel, cavity-like changes are seen within the retina, but retinal thickness does not increase; rather, it decreases. Diabetic macular edema is accompanied by retinal thickening. The difference in retinal thickness on OCT is the most important distinguishing feature.10)
For type 1, direct laser photocoagulation of capillary microaneurysms is the first-line treatment. However, recurrence is common, and coagulation may be difficult if the microaneurysms are close to the foveal avascular zone. In some cases, good visual outcomes occur without treatment, and spontaneous resolution of macular edema has been observed. Therefore, careful management is required unless there is progressive vision loss. There is no consensus on local injections of triamcinolone or VEGF inhibitors.
For the non-proliferative stage of type 2, there is currently no established standard treatment. 10)Retinal photocoagulation is ineffective. Intravitreal anti-VEGF injections have also shown no benefit in the non-proliferative stage, and it has been suggested that they may inhibit the neuroprotective effects of VEGF. 5) The efficacy of intravitreal steroid injections has not been confirmed.
The CNTF implant (ENCELTO) has emerged as the first treatment option for type 2 MacTel. For details, see the section “Latest Research and Future Prospects”.
QIs there a treatment for the non-proliferative stage of MacTel Type 2?
A
Currently, there is no established standard treatment. Retinal photocoagulation is ineffective, and anti-VEGF drugs are not recommended in the non-proliferative stage because they may inhibit neuroprotective effects. 10) The ENCELTO implant, which releases CNTF, has been shown in phase 3 trials to slow the progression of ellipsoid zone loss, and it is expected to be a future option.
In the proliferative stage, intravitreal anti-VEGF injections are the mainstay of treatment. 1)19) Transpupillary thermotherapy (TTT) and photodynamic therapy (PDT) have also been reported to be effective, but anti-VEGF drugs are currently the first-line treatment. 10)
Gonzalez Martinez et al. (2023) reported a case of a 54-year-old woman with type 2 MacTel complicated by choroidal neovascularization, who received 18 anti-VEGF injections (15 bevacizumab and 3 aflibercept) over 2 years, achieving stabilization of the neovascular membrane and maintenance of visual acuity at 20/30. 1)
Moussa et al. (2021) reported a case of an 11-year-old patient with proliferative type 2 MacTel who received PRN aflibercept (2 mg/0.05 mL) injections. After 5 injections, the neovascularization regressed and visual acuity improved by 5 lines. SS-OCT-A was useful for noninvasive diagnosis and follow-up. 5)
Chronic neovascular membranes can lead to scarring and reduced treatment response, so early treatment is important for improving visual prognosis. 1)
For full-thickness macular holes associated with type 2 MacTel, vitrectomy (internal limiting membrane peeling + gas tamponade) may be performed, but the closure rate is lower and postoperative visual acuity is poorer compared to typical macular holes. 10)
Chandra et al. (2021) reported a case of type 2 MacTel with a nearly full-thickness macular hole accompanied by an ILM drape that closed spontaneously. Restoration of the external limiting membrane (ELM) enabled hole closure, and visual acuity in the left eye recovered to 20/40 over 32 months of follow-up. In the presence of an ILM drape, conservative observation may be an option. 9)
The pathogenesis of type 2 MacTel was traditionally thought to be primarily vascular, but it is now widely believed that Müller cell degeneration is the origin of the disease, and telangiectasia is a secondary change. 10)
Gass proposed that Müller cells and parafoveal neurons are the first structures affected. Histopathological studies have confirmed depletion of Müller cells in the parafovea of patients with type 2 MacTel. 18)
Müller cells are the major glial cells spanning the full thickness of the retina and perform the following functions:
Maintenance of the blood-retinal barrier: Involved in barrier formation, especially at the deep capillary plexus level
Formation of the internal limiting membrane (ILM) and external limiting membrane (ELM): The basement membrane of Müller cells is a major component
Storage of macular pigment (xanthophyll): Loss of pigment is an indicator of Müller cell dysfunction
Neuroprotection and metabolic support: Production of trophic factors including VEGF
It is thought that dysfunction of Müller cells leads to breakdown of the blood-retinal barrier, abnormal VEGF production, and reduced nutrient supply to photoreceptors, resulting in capillary dilation, neovascularization, and photoreceptor degeneration. 1)
GWAS studies have identified an association between MacTel 2 and loci in the glycine/serine metabolism pathway. 3) Macular Müller cells are particularly dependent on serine biosynthesis, and impairment of this pathway leads to vulnerability to oxidative stress. 3) Reduced serine leads to accumulation of neurotoxic 1-deoxysphingolipids, promoting retinal neurodegeneration.
The disease is thought to progress through the following stages:
Stage 1: Müller cell degeneration → loss of xanthophyll → iso-reflective and hyper-autofluorescent appearance on fundus autofluorescence10)
Stage 2: Telangiectasia of the deep capillary plexus → appearance of IDZ changes 2)
Stage 3: Loss of the ellipsoid zone → atrophy and cavitation of the outer retina
Stage 4: Proliferation and intraretinal migration of RPE
Stage 5: Abnormal VEGF production → subretinal neovascularization and retinal-choroidal anastomosis
In a longitudinal study by Chandran et al. (2023), sequential outer retinal changes were confirmed: IDZ attenuation → IDZ loss → EZ attenuation → EZ loss. 2) The annual progression rate of IDZ loss was 142–172 μm/year, and EZ attenuation was approximately 83 μm/year.
Differences in pathology between type 1 and type 2
The primary lesion sites are fundamentally different. Type 1 is mainly characterized by leakage of plasma components due to vascular damage, whereas type 2 primarily involves atrophic changes in the outer retinal layers. This difference determines the OCT findings (type 1: retinal thickening; type 2: retinal thinning).
QWhy is MacTel bilateral?
A
In type 2 MacTel, genetic factors and systemic metabolic abnormalities (abnormalities in serine metabolism and sphingolipid metabolism) are involved in the pathogenesis, so Müller cells in both eyes are similarly affected. 3) The genetic variants in the glycine/serine metabolism pathway identified by GWAS are systemic factors, unlike local factors that affect only one eye.
7. Latest Research and Future Prospects (Investigational Stages)
ENCELTO is an encapsulated cell-based gene therapy consisting of allogeneic RPE cells engineered to secrete recombinant human ciliary neurotrophic factor (rhCNTF). It activates protective signaling pathways that promote photoreceptor survival.
Results from two randomized, multicenter, double-masked, sham-controlled phase 3 trials have been reported.
Trial 1 (n=115): The EZ loss area over 24 months was 0.075 mm² in the treatment group vs 0.166 mm² in the sham group, achieving approximately 55–56% slowing of progression (p<0.0001). Significant differences were also observed in total retinal sensitivity of the EZ defect area.
Trial 2 (n=113): The EZ loss area was 0.111 mm² vs 0.160 mm², approximately 30–31% slowing of progression (p=0.0186). However, no significant difference was found in retinal sensitivity.
The main adverse events compared to the sham group were higher frequencies of subconjunctival hemorrhage (31%), delayed dark adaptation (23.1%), suture-related complications (15.4%), and vitreous hemorrhage (8.5%). Serious events were rare.
Serine supplementation therapy and therapeutic approaches targeting sphingolipid metabolism regulation are under investigation. 3) In iPSC-derived RPE cell models, low serine levels and mitochondrial dysfunction have been reproduced in cells from MacTel 2 patients, advancing the understanding of pathology and the search for therapeutic targets. 3)
Halouani et al. (2024) reported a case of bilateral MacTel 2 in a 49-year-old woman with Down syndrome. 3) Abnormalities in serine/glycine metabolism and sphingolipid (ceramide) metabolism have been implicated in both conditions, suggesting a possible common metabolic pathway disorder. With the increased life expectancy of Down syndrome patients, the importance of adult retinal screening is growing.
Moir et al. (2022) reported that OCT-A is useful in the diagnosis and management of atypical cases of type 2 MacTel. 7) In particular, capillary dilation in the DCP is the earliest vascular change detected by OCT-A, and it is important that deep vascular changes, which are difficult to evaluate with FA, can be visualized noninvasively.
Gonzalez Martinez OG, Ayala Rodríguez SC, Pappaterra-Rodriguez M, Requejo-Figueroa G, Oliver AL. Intravitreal Bevacizumab for Choroidal Neovascular Membrane in Macular Telangiectasia Type 2. Cureus. 2023;15(6):e40528. doi:10.7759/cureus.40528. PMID:37461786; PMCID:PMC10350322.
Chandran K, Giridhar A, Gopalakrishnan M, Sivaprasad S.. Relation of interdigitation zone changes and right-angle vessels in Macular Telangiectasia Type-2 (MacTel). Eye (Lond). 2023;37(14):2977-2986. doi:10.1038/s41433-023-02453-8. PMID:36841866; PMCID:PMC10516857.
Halouani S, Miere A, Le HM, Herda N, Cirneanu A, Souied EH.. Macular telangiectasia type 2 in a patient with Down syndrome: A possible association. Am J Ophthalmol Case Rep. 2024;36:102173. doi:10.1016/j.ajoc.2024.102173. PMID:39319206; PMCID:PMC11421271.
Ramamurthy SR, Dave VP.. Macular telangiectasia type 2 presenting with sub-internal limiting membrane hemorrhage. Taiwan J Ophthalmol. 2025;15(3):491-493. doi:10.4103/tjo.tjo-d-23-00033. PMID:40995325; PMCID:PMC12456921.
Magdy Moussa, Mahmoud Leila, Omar Moussa. Multimodal imaging of macular telangiectasia type 2 in a pediatric patient. American Journal of Ophthalmology Case Reports. 2021;22:101082. doi:10.1016/j.ajoc.2021.101082.
Zerbinopoulos B, Goman-Baskin E, Greenberg PB, Bryan R, Messina C.. The Role of Diagnostic Imaging in Macular Telangiectasia Type 2. Fed Pract. 2021;38(12):594-597. doi:10.12788/fp.0200. PMID:35177889; PMCID:PMC8843004.
Moir J, Amin SV, Khanna S, Komati R, Shaw LT, Dao D, et al. Use of OCT Angiography to Diagnose and Manage Atypical Presentations of Macular Telangiectasia Type 2. International journal of molecular sciences. 2022;23(14). doi:10.3390/ijms23147849. PMID:35887197; PMCID:PMC9321649.
Erdem A, Duyan SA. Tamoxifen Retinopathy and Macular Telangiectasia Type 2: Case-Based Differential Diagnosis. Beyoglu eye journal. 2025;10(4):254-257. doi:10.14744/bej.2025.97355. PMID:41658254; PMCID:PMC12875193.
Chandra V, Merani R, Hunyor AP, Gillies M. Spontaneous Closure of a Macular Hole in Macular Telangiectasia Type 2. Journal of vitreoretinal diseases. 2021;5(3):275-280. doi:10.1177/2474126420958907. PMID:37006519; PMCID:PMC9979038.
J. Donald M. Gass. A Fluorescein Angiographic Study of Macular Dysfunction Secondary to Retinal Vascular Disease. Arch Ophthalmol. 1968;80(5):592. doi:10.1001/archopht.1968.00980050594005.
Gass JD, Blodi BA. Idiopathic juxtafoveolar retinal telangiectasis. Update of classification and follow-up study. Ophthalmology. 1993;100:1536-1546. doi:10.1016/s0161-6420(93)31447-8.
Lawrence A. Yannuzzi. Idiopathic Macular Telangiectasia. Arch Ophthalmol. 2006;124(4):450. doi:10.1001/archopht.124.4.450.
Clemons TE, Gillies MC, Chew EY, Bird AC, Peto T, Figueroa MJ, et al. Baseline characteristics of participants in the natural history study of macular telangiectasia (MacTel) MacTel Project Report No. 2. Ophthalmic epidemiology. 2010;17(1):66-73. doi:10.3109/09286580903450361. PMID:20100102; PMCID:PMC8329604.
Clemons TE, Gillies MC, Chew EY, Bird AC, Peto T, Wang JJ, Mitchell P, Ramdas WD, Vingerling JR; Macular Telangiectasia Project Research Group. Medical characteristics of patients with macular telangiectasia type 2 (MacTel Type 2) MacTel Project Report No. 3. Ophthalmic Epidemiol. 2013 Apr;20(2):109-113. doi:10.3109/09286586.2013.766757. PMID:23510315.
Heeren TFC, Chew EY, Clemons T, Fruttiger M, Balaskas K, Schwartz R, et al. Macular Telangiectasia Type 2: Visual Acuity, Disease End Stage, and the MacTel Area: MacTel Project Report Number 8. Ophthalmology. 2020;127(11):1539-1548. doi:10.1016/j.ophtha.2020.03.040. PMID:32586743; PMCID:PMC8380038.
Maruko I, Iida T, Sugano Y, Ojima A, Oyamada H, Sekiryu T.. Demographic features of idiopathic macular telangiectasia in Japanese patients. Jpn J Ophthalmol. 2012;56(2):152-158. doi:10.1007/s10384-011-0112-5. PMID:22219035.
Powner MB, Gillies MC, Tretiach M, et al. Perifoveal Muller cell depletion in a case of macular telangiectasia type 2. Ophthalmology. 2010;117:2407-2416.
Narayanan R, Chhablani J, Sinha M, Dave V, Tyagi M, Pappuru RR, et al. Efficacy of anti-vascular endothelial growth factor therapy in subretinal neovascularization secondary to macular telangiectasia type 2. Retina (Philadelphia, Pa.). 2012;32(10):2001-5. doi:10.1097/IAE.0b013e3182625c1d. PMID:22990322.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.