Fluorescein (fluorescein): A fluorescent dye that emits green fluorescence when excited by blue light. It is the most widely used
Rose bengal (rose bengal): A dye that stains dead cells, degenerated cells, and mucus red
Lissamine green (lissamine green): A substitute dye with staining properties similar to rose bengal but less irritation
The main purposes of this test are as follows:
To detect and quantify corneal and conjunctival epithelial damage in dry eye
To assess the extent of corneal infiltration and ulcers in infectious keratitis2)
To evaluate epithelial damage caused by drug toxicity, contact lens–related injury, eyelid abnormalities, and similar conditions
To support the diagnosis of Sjögren syndrome (van Bijsterveld scoring)3)
In the 2016 Dry Eye Clinical Practice Guideline, evaluation combining tear film breakup time (BUT) measurement and fluorescein staining is recommended as a core part of dry eye diagnosis1). In the 2006 edition, corneal and conjunctival epithelial damage was essential for diagnosing dry eye, but in the 2016 edition, epithelial damage was no longer a required criterion, and diagnosis shifted to short BUT and symptoms. Even so, vital staining remains an important way to objectively record the degree and pattern of epithelial damage1).
In the initial evaluation of infectious keratitis, fluorescein staining is also a standard procedure used to understand the extent and shape of corneal epithelial defects, and it is incorporated into care based on the Infectious Keratitis Clinical Practice Guideline (3rd edition)2).
QWhat can a vital staining test show?
A
The distribution and severity of corneal and conjunctival epithelial damage are visualized. With fluorescein, punctate superficial keratopathy (SPK) and erosions or ulcers of the corneal epithelium appear as fluorescence, and with rose bengal or lissamine green, dead and degenerated cells are stained. The pattern of SPK distribution can help suggest the underlying condition (dry eye, drug toxicity, contact lens-related injury, and so on). Scoring methods can also be used to quantify the damage and track treatment effects over time.
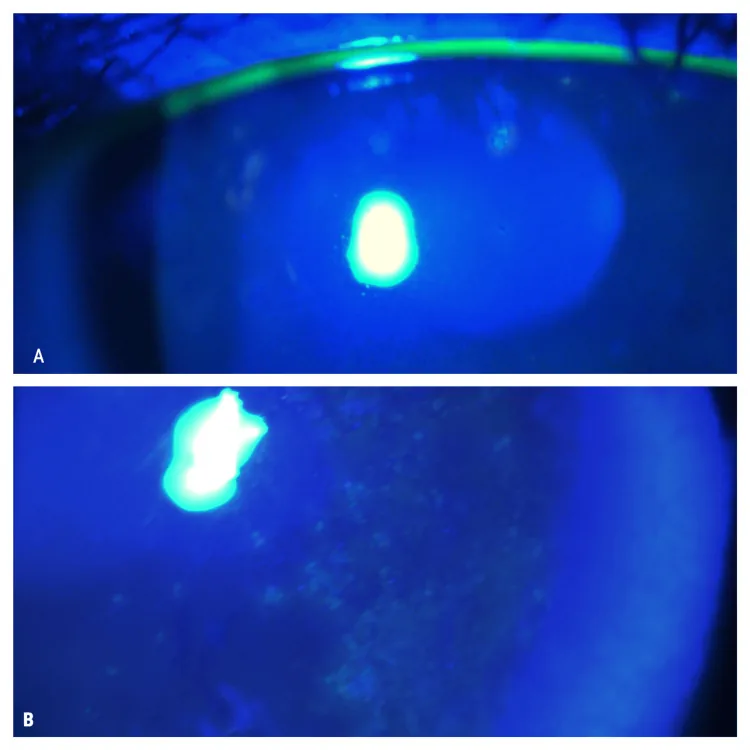
Tagmouti A, Lazaar H, Benchekroun M, Boutaj T, Benchekroun S, Amazouzi A, et al. Association Between Thygeson Superficial Punctate Keratitis and Celiac Disease. Cureus. 2025;17(3):e80252. doi:10.7759/cureus.80252. PMID:40196095; PMCID:PMC11975144. Figure 2. PMID: 40196095; PMCID: PMC11975144; DOI: 10.7759/cureus.80252. License: CC BY.
With slit-lamp fluorescein staining, corneal epithelial lesions in the right eye (A) and left eye (B) are shown as green fluorescence under blue light. This corresponds to the fluorescein staining observation method covered in the section on characteristics and procedure of each dye.
Fluorescein is the most widely used vital dye. It is commonly used because it is easy to obtain, safe, and causes little irritation. Fluorescein is a dye that emits green fluorescence (521 nm) when excited by blue light (maximum absorption wavelength 494 nm). It can be observed with only a cobalt blue filter, but lesions are shown more clearly when a blue-free filter is added to the observation system.
Staining principle and key observation points:
Penetrates and stains areas where tight junctions between epithelial cells are disrupted
The clearest observation is possible with a combination of a cobalt blue filter (excitation 494 nm) and a blue-free filter (barrier filter)
Staining target: areas where tight junctions between epithelial cells are disrupted (intercellular spaces)
Main uses: SPK detection, BUT measurement, corneal ulcer/erosion evaluation
Irritation: low (easiest to use)
Observation filter: cobalt blue + blue-blocking (barrier) filter
Rose bengal
Staining color: red
Stained targets: dead cells, degenerated cells, areas lacking mucin protection
Main use: diagnosis of Sjögren syndrome (van Bijsterveld score), dry eye evaluation
Irritation: strong (pain when instilled)
Observation filter: white light or red filter
Lissamine green
Staining color: green
Stained targets: dead cells, degenerated cells (same mechanism as rose bengal)
Main use: alternative to rose bengal. Dry eye and Sjögren syndrome evaluation
Irritation: low (less burden for patients than rose bengal)
Observation filter: clearly seen with a red filter (560 nm or above)
Characteristic
Fluorescein
Rose bengal
Lissamine green
Staining color
Green fluorescence
Red
Green
Staining target
Intercellular spaces (areas where tight junctions are disrupted)
Dead cells, degenerated cells, and mucin-deficient areas
Dead cells and degenerated cells
Irritation
Low
High (with pain)
Low
Observation filter
Cobalt blue + blue-free
White light · red filter
Red filter (560 nm or higher)
Main uses
SPK · BUT measurement · corneal ulcer
Sjögren diagnosis · dry eye
Rose bengal alternative
Representative score
Oxford score / NEI score
van Bijsterveld score
van Bijsterveld score
QWhat is the difference between rose bengal and lissamine green?
A
Both stain dead and degenerated cells, but lissamine green is less irritating and easier on patients. Rose bengal can cause pain when instilled, so in some cases topical anesthesia may be needed. Lissamine green has become more widely used in recent years as an alternative dye that solves these drawbacks. For observation, using a red filter (560 nm or higher) makes the stained areas easier to see clearly.
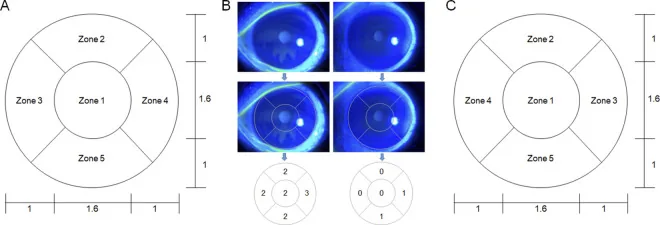
Kim S, Park D, Shin Y, et al. Deep learning-based fully automated grading system for dry eye disease severity. PLoS One. 2024;19(3):e0299776. Figure 1. PMID: 38483911; PMCID: PMC10939279; DOI: 10.1371/journal.pone.0299776. License: CC BY 4.0.
An evaluation grid that divides the cornea into five regions—central, superonasal, superotemporal, inferonasal, and inferotemporal—based on the NEI score, along with an example evaluation using actual fluorescein staining photographs. This corresponds to the NEI/Industry Workshop score covered in the section ‘Scoring methods and criteria’ of the main text.
Several scoring systems have been established to quantify corneoconjunctival epithelial damage.
Evaluate each of the three areas—cornea, nasal bulbar conjunctiva, and temporal bulbar conjunctiva—on a 0 to 3 scale (0: no staining, 1: a few punctate stains, 2: staining tending to merge, 3: widespread staining). A total score of 3.5 or higher is considered abnormal and is internationally adopted as a diagnostic criterion for Sjögren syndrome3).
Each of the three areas—cornea and bulbar conjunctiva (nasal and temporal)—is scored from 0 to 4 in five grades, for a total of 15 points. Each grade is assessed semiquantitatively by comparing it with panel diagrams. It is used to assess dry eye severity and treatment response.
The cornea is divided into five zones—central, superonasal, superotemporal, inferonasal, and inferotemporal—and each zone is scored from 0 to 3, for a total of 15 points. It is widely used in clinical research and multicenter trials.
Staining criteria for corneal and conjunctival epithelial damage in the Dry Eye Clinical Practice Guidelines (2006 edition)1):
fluorescein staining score of 3 or higher
or rose bengal staining score of 3 or higher
or lissamine green staining score of 3 or higher
In the 2016 dry eye diagnostic criteria, epithelial damage was removed from the essential diagnostic requirements, but observing epithelial damage continues to play an important role in assessing dry eye severity and treatment response1).
4. Clinical significance and how to read staining patterns
Punctate superficial keratopathy (superficial punctate keratopathy: SPK) is the most common eye finding in patients who complain of a foreign body sensation. SPK is a “result” of corneal epithelial damage caused by some underlying factor, not a diagnosis of the cause. Fluorescein vital staining is essential for detecting SPK and understanding its distribution pattern, and it can reveal subtle SPK that cannot be seen with slit-lamp microscopy alone.
When SPK is detected, it is important to actively infer the underlying cause from its distribution pattern.
In drug-induced toxic keratopathy, damage to the conjunctival epithelium is less pronounced than damage to the corneal epithelium. This finding can be clearly confirmed with fluorescein staining and is useful for distinguishing it from other causative diseases. If diffuse SPK is seen across the entire cornea, the effect of the eyedrops being used (preservatives, high-concentration medications, aminoglycoside antibiotics, etc.) should be considered2).
The significance of staining in infectious keratitis
In infectious keratitis, fluorescein staining allows objective assessment of the shape, area, and depth (judged by the intensity of staining) of corneal epithelial defects. The extent and shape of the ulcer are used as indicators for choosing treatment and for follow-up observation2). In addition, antibacterial eyedrops (high-concentration formulations and aminoglycosides) are likely to cause corneal epithelial toxicity, so it is important to check with vital staining during treatment for any worsening of epithelial damage2).
QWhat can staining patterns tell us?
A
By observing the distribution pattern of SPK, the underlying disease can be inferred. SPK concentrated in the lower cornea suggests dry eye or entropion, upper SPK suggests SLK or trachoma, and diffuse SPK throughout the cornea suggests drug toxicity or viral keratitis. SPK at the 3 to 9 o’clock position is typical of contact lens injury, and SPK in the central cornea is characteristic of lagophthalmos and neuroparalytic keratitis. SPK is only the “result” of epithelial damage, and using the distribution pattern as a clue to search for the cause is the key point in care.
5. Related treatment guidelines (management by cause of epithelial damage)
Standard treatment based on the Dry Eye Clinical Practice Guidelines (2016 edition) is as follows1).
3% diquafosol sodium eye drops (Diquas®): instill 6 times a day. It has multifaceted effects, including promoting aqueous secretion, promoting secretion of secretory mucin (MUC5AC), and increasing expression of membrane-associated mucins (MUC1, MUC4, MUC16). It improves tear film stability, corneoconjunctival epithelial damage, and subjective symptoms
2% rebamipide suspension eye drops (Mucosta®): instill 4 times a day. They promote secretion of secretory mucin and increase expression of membrane-associated mucin by increasing the number of goblet cells. They improve corneoconjunctival epithelial damage and subjective symptoms
0.1% hyaluronic acid eye drops: improve corneoconjunctival epithelial damage and subjective symptoms. Can be used for a broad range of subtypes
Punctal plug insertion: suppresses tear drainage. It is the first-line choice in the area break pattern (tear-deficient type)
Based on the Infectious Keratitis Clinical Practice Guidelines (3rd edition), select the appropriate antimicrobial agent after identifying the causative organism2).
Initial treatment of bacterial keratitis: broad-spectrum fluoroquinolone eye drops such as levofloxacin 1.5%
Note that high-concentration eye drops and aminoglycosides are prone to causing corneal epithelial damage2)
During treatment, regularly confirm improvement in epithelial damage with vital staining
Fluorescein is a fluorescent dye that absorbs cobalt blue light (494 nm) and emits green fluorescence (521 nm). The principle of fluorescence is photoluminescence, in which absorbed energy is re-emitted as light.
A blue-blocking filter (barrier filter) blocks the excitation light (around 494 nm) and lets only the fluorescence wavelength (521 nm) pass. This removes background light and makes SPKfluorescein staining easier to see. When a blue-blocking filter is attached to the slit lamp microscope, the sensitivity for detecting SPK improves greatly compared with using the cobalt blue filter alone.
When the tight junctions of the corneal epithelium break down, fluorescein penetrates the intercellular spaces and fluoresces. Areas where normal tight junctions are intact do not allow fluorescein to enter and therefore are not stained.
Rose bengal selectively stains cells that are not protected by mucin. Healthy ocular surface cells are covered by a mucin layer (mainly secretory mucin MUC5AC), which prevents rose bengal staining. Dead and degenerated cells have lost this mucin protection, so they are stained. Unlike fluorescein, it stains the dead cells themselves, so it can be considered an indicator of ocular surface cell viability.
Lissamine green stains dead and degenerated cells by a mechanism similar to rose bengal. Staining can be seen most clearly under observation with a red filter (560 nm or higher). It is thought to be less irritating to the ocular surface than rose bengal because of differences in penetration into living tissue.
The blue filter is especially important for fluorescein observation. Even with cobalt blue light without a filter, lesions can be seen, but adding a blue filter:
removes background light (scattered cobalt blue light)
allows only fluorescent wavelengths to reach the retina, greatly improving contrast
makes fine SPK easier to detect
also improves the accuracy of BUT measurement (assessment of tear film breakup)
Noninvasive corneal epithelial thickness mapping with anterior segment OCT: Advances are being made in tomographic mapping of corneal epithelial thickness using anterior segment optical coherence tomography (AS-OCT). It may make it possible to evaluate thinning and irregular distribution of the corneal epithelium without vital staining, and research is underway as a complement or alternative to vital staining4)
Objectifying stain scores with automated image analysis: Stain scoring (Oxford score, van Bijsterveld score, etc.) currently depends on the observer’s subjective judgment. Development of automated scoring systems using AI and machine learning is progressing, and improved reproducibility and objectivity are expected5)
Research to refine staining sensitivity and specificity: Studies are ongoing to evaluate the sensitivity and specificity of each stain dye by dry eye subtype and disease stage. In particular, comparisons of the equivalence and interchangeability of lissamine green and rose bengal are being conducted
Combination with confocal microscopy: By combining in vivo confocal microscopy (IVCM) with vital staining, cellular-level evaluation of epithelial damage is becoming possible. Its application to identifying pathogens in infectious keratitis is also being studied4)
Vitali C, Bombardieri S, Jonsson R, Moutsopoulos HM, Alexander EL, Carsons SE, Daniels TE, Fox PC, Fox RI, Kassan SS, Pillemer SR, Talal N, Weisman MH, European Study Group on Classification Criteria for Sjögren’s Syndrome. Classification criteria for Sjögren’s syndrome: a revised version of the European criteria proposed by the American-European Consensus Group. Ann Rheum Dis. 2002;61(6):554-558. doi:10.1136/ard.61.6.554. PMID:12006334; PMCID:PMC1754137.
Palakkamanil MM, Nichols KK. Comparison of lissamine green and rose bengal staining. Optom Vis Sci. 2015;92(5):566-571.
Bron AJ, Evans VE, Smith JA. Grading of corneal and conjunctival staining in the context of other dry eye tests. Cornea. 2003;22(7):640-50. doi:10.1097/00003226-200310000-00008. PMID:14508260.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.