Pediatric penetrating keratoplasty (PKP) is a full-thickness corneal transplantation performed in patients under 18 years of age. It aims to replace the opaque full-thickness cornea with a donor cornea to improve vision or maintain ocular structure.
The frequency of indications varies by region. Congenital opacities account for 14–64%, acquired non-traumatic diseases (e.g., keratoconus, post-infectious scars) for 19–80%, and traumatic opacities for 6–29% 1. A 15-year single-center report from the Middle East found progressive keratoconus to be the most common (55.7%), followed by traumatic opacities (15.4%) 2.
The critical period for visual development is 2–6 months of age, and it is even shorter for unilateral opacities. Among pediatric corneal specialists, surgical intervention at 1–3 months of age is recommended. However, recent case series show that age at surgery does not significantly affect graft survival, while glaucoma and concurrent surgeries have a stronger impact on prognosis 3.
In recent years, DSEK (Descemet stripping endothelial keratoplasty) and DALK (deep anterior lamellar keratoplasty) have been successfully performed in children for specific diseases, expanding alternatives to full-thickness transplantation 1.
QHow is pediatric corneal transplantation different from adult transplantation?
A
Compared to adults, children have lower scleral rigidity, increasing the risk of intraoperative globe collapse. Postoperative inflammation is stronger, and suture loosening due to tissue contraction is more common. Graft failure rates are higher than in adults, and amblyopia management is necessary. General anesthesia is mandatory, and ensuring compliance with postoperative eye drops is also a challenge.
Peters anomaly: Defect of corneal endothelium, Descemet membrane, and part of the stroma, presenting with central disc-shaped opacity. Approximately 80% are bilateral, and 50–70% are complicated by glaucoma4.
Sclerocornea: A congenital anomaly in which the peripheral or entire cornea appears scleral-like and opaque.
CHED: Congenital hereditary endothelial dystrophy. Bilateral corneal edema and opacity present from birth.
Birth trauma: Descemet membrane rupture due to forceps delivery. Usually unilateral (more common in the left eye), leaving vertical linear opacity and astigmatism.
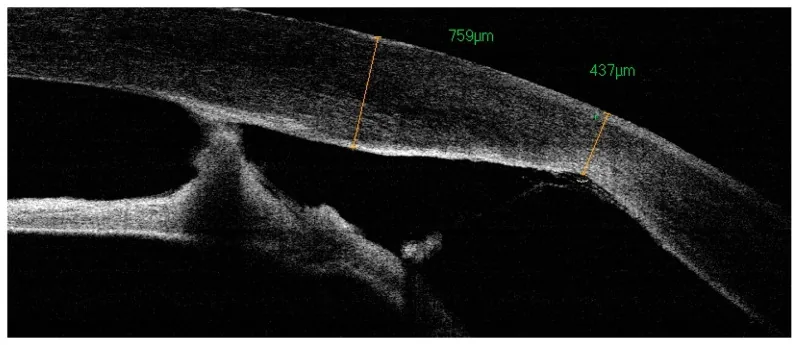
J Clin Med. 2024 Jan 17; 13(2):532. Figure 3. PMCID: PMC10816361. License: CC BY.
Anterior segment OCT shows the corneal contour after transplantation, the junction with the host side, and peripheral iris adhesion. This corresponds to the anterior segment OCT evaluation after pediatric corneal transplantation discussed in the section “Diagnosis and Examination Methods.”
Slit-lamp microscopy: Evaluate the extent and depth of corneal opacity, presence of angle adhesion, and limbal function. In infants, examination under general anesthesia (EUA) may be required.
Carefully assess whether the benefits of penetrating keratoplasty outweigh the risks. Consider alternative procedures (endothelial keratoplasty, deep lamellar keratoplasty) or partial iridectomy.
For unilateral corneal opacity, observation without surgery is an option. Some surgeons do not recommend surgery for unilateral disease due to difficulty in postoperative management and low success rates. On the other hand, some emphasize the importance of securing binocular vision.
Explain thoroughly to the guardians that frequent postoperative steroid eye drops (every hour for the first few days) and frequent clinic visits are required.
The donor graft is made 0.5–1 mm larger than the host cornea. Suturing is performed using 10-0 nylon with interrupted sutures, continuous sutures, or a combination. The procedure is performed under general anesthesia, avoiding the use of succinylcholine and ketamine.
Children exhibit a stronger inflammatory response than adults. Increased fibrin release can lead to iridocorneal adhesions. Loosening of sutures due to tissue contraction can cause suture abscesses and neovascularization, leading to rejection and graft failure1. In fact, a single-center study in Jordan reported that loose sutures were the most common postoperative complication (31.5%), followed by rejection (15.4%)2.
Steroid eye drops: Initiated every hour in the early postoperative period and tapered very slowly. One approach is to start betamethasone 0.1% about 5 times daily and taper over approximately 3 months1
Antibiotics: Used for a longer duration than in adults1
Suture management: Instruct caregivers to observe the cornea daily with a penlight. In infants, suture removal begins 2 weeks postoperatively and is completed in about 3 months1
Amblyopia treatment: Begin vision training as soon as possible after surgery. Amblyopia treatment has been reported as the only independent prognostic factor for postoperative visual improvement1
Examination under general anesthesia: Frequent postoperative fundus examinations and consultations are necessary1
QWhat precautions are needed after surgery?
A
In the early postoperative period, hospital visits are required at least 2–3 times per week, then once a week for several months. Parents should observe the cornea daily with a penlight and promptly consult a doctor if they find loosening of sutures or new infiltrates. It is important to continue steroid eye drops as instructed and not to discontinue them on your own. Avoid rubbing the eyes, and amblyopia treatment should be performed concurrently.
The prognosis of pediatric penetrating keratoplasty is guarded, with lower success rates than in adults. The main causes of graft failure are rejection and infection1. Systematic reviews report rejection rates in children ranging from 22% to 43.4%, with some reports reaching up to approximately 50%1. Even if the graft remains clear, poor visual acuity due to amblyopia occurs at a high rate1.
Relatively good outcomes are obtained in acquired corneal opacities, with 1-year clear graft survival rates of approximately 76–80% reported in mixed cohorts including traumatic opacities23. In contrast, congenital corneal opacities have a poor prognosis; in Peters anomaly, 42.5% maintain clarity, and the survival probability of 52% at 6 months decreases to 22% at 2 years4. In a 5-year follow-up study of congenital opacities in children under 3 years of age, the 12-month survival rate was 83.3%, the 18-month survival rate was 66.7%, and the final survival rate was only 50%5. In Peters anomaly, 65% of graft failures were due to rejection, and 93.3% of these occurred within the first year after surgery4.
Glaucoma comorbidity is an important poor prognostic factor, with 1-year graft survival rates of 51.9% with glaucoma and 90.7% without glaucoma3.
QWhat is the success rate of surgery?
A
The success rate of pediatric PK depends largely on the underlying disease and the presence of glaucoma. While the 1-year clear graft survival rate in mixed cohorts is reported to be approximately 76–80%23, in Peters anomaly the clear graft survival rate is only 42.5%4. When glaucoma is present, the 1-year survival rate drops to about half (51.9%)3. Furthermore, even if the graft is clear, visual improvement may not be achieved due to amblyopia, and amblyopia treatment has been reported as the only independent prognostic factor for postoperative visual improvement1.
Peters anomaly results from abnormal migration of neural crest cells after the 6th week of gestation. The corneal endothelium, Descemet’s membrane, and part of the corneal stroma are absent, leading to a central disc-shaped opacity. It may be accompanied by iridocorneal adhesions (type 1) or lens-corneal adhesions (types 2 and 3). Glaucoma is present in approximately 50–70% of cases4.
Sclerocornea results from abnormal differentiation of the cornea and sclera during development. The peripheral or entire cornea appears sclera-like, and the limbus becomes indistinct.
CHED is caused by dysfunction of corneal endothelial cells, leading to bilateral corneal edema and opacity present at birth.
The reasons for higher graft failure rates in children compared to adults are as follows.
Children have a more active immune response than adults, resulting in a higher frequency of endothelial rejection1. Endothelial rejection is characterized by localized keratic precipitates on the graft and a Khodadoust line (rejection line), accompanied by stromal edema. If detection is delayed, graft function may be irreversibly lost.
Additionally, because wound healing is more active in children, tissue contraction tends to occur at the graft-host junction. This contraction can cause sutures to loosen, and loose sutures may become a nidus for infection or trigger rejection12.
Gurnani B, Kaur K, Chaudhary S, et al. Pediatric corneal transplantation: techniques, challenges, and outcomes. Therapeutic Advances in Ophthalmology. 2024;16. PMID: 38533487. PMCID: PMC10964464. PMC全文
Abukahel A, Aldiwanie AS, AlRyalat SA, Gharaibeh AM. Indications and Outcomes of Pediatric Penetrating Keratoplasty: A Retrospective Observational Study. Med Hypothesis Discov Innov Ophthalmol. 2022;11(3):103-114. PMID: 37641699. PMCID: PMC10445322. PMC全文
Karadag R, Chan TCY, Azari AA, Nagra PK, Hammersmith KM, Rapuano CJ. Survival of Primary Penetrating Keratoplasty in Children. Am J Ophthalmol. 2016;171:95-100. PMID: 27590122. PubMed
Rao KV, Fernandes M, Gangopadhyay N, Vemuganti GK, Krishnaiah S, Sangwan VS. Outcome of penetrating keratoplasty for Peters anomaly. Cornea. 2008;27(7):749-753. PMID: 18650657. PubMed
Susiyanti M, Mawarasti B, Manurung FM. Penetrating keratoplasty in children under 3 years old with congenital corneal opacities. Int J Ophthalmol. 2022;15(1):75-79. PMID: 35047355. PMCID: PMC8720356. PMC全文
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.