Intracorneal ring segment (ICRS) extrusion is a complication that can occur after ICRS implantation. Progressive corneal stromal thinning and epithelial breakdown lead to the ring protruding from the corneal surface.
ICRS extrusion is the most common cause requiring ring removal, accounting for 48.2% of all removal cases. The average onset time is about 10 years, but it can occur at any time from 1 month to 20 years after implantation.
Prior to ICRS extrusion, ring migration or corneal melting is frequently observed. It presents with foreign body sensation, photophobia, and epithelial defects, and findings resolve after ring removal.
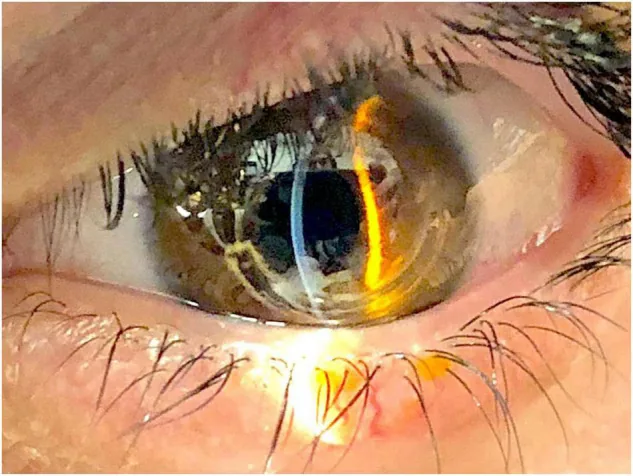
Raffaele Nuzzi et al. A Combined Procedure of Intrastromal Corneal Rings Explantation and Penetrating Keratoplasty in a Patient With Keratoconus: A Case Report. Frontiers in Medicine. 2022 Mar 11; 9:853702. Figure 1. PMCID: PMC8961690. License: CC BY.
Slit-lamp photograph of ICRS extrusion. The ring segment is protruding from the corneal surface.
Foreign body sensation is the most common symptom. It may be accompanied by photophobia, tearing, and itching. A history of prior eye rubbing or trauma may be elicited.
Diagnostic features include the following three: presence of an area of stromal thinning, epithelial defect, and ring protrusion (sometimes linear ring exposure without protrusion).
Preceding corneal melting, ring migration, or anterior stromal necrosis are signs of impending extrusion. Epithelial defects disappear after removal but do not resolve with contact lens cessation alone. They present with punctate, arcuate, or linear staining patterns. Tunnel neovascularization may occur with superficial corneal neovascularization.
Eccentric cone + grade 3 keratoconus increases risk of migration and melting
Narrow ICRS channels (6.6 mm × 7.6 mm) are more prone to ring migration with epithelial plugs and tunnel opacities compared to wide tunnels (6.7 mm × 8.2 mm).
General ICRS complications include infection, vision loss, intraoperative perforation, postoperative segment extrusion/migration, epithelial defects, corneal scarring, and corneal melting 1). Intralamellar tunnel deposits are seen in up to 74% but have little impact on visual function 1).
QHow can ICRS extrusion be prevented?
A
There are three main preventive measures. First, adhere to the “pachymetry rule” and keep the ring thickness less than half the corneal thickness at the implantation site. Second, use a femtosecond laser to accurately create a tunnel with a channel depth of 80%. Third, place the ring tip away from the incision. Postoperatively, it is also important to confirm early ring position stability with CAS-OCT.
ICRS extrusion is diagnosed based on clinical findings. The diagnostic criteria include stromal thinning, ring protrusion through an epithelial defect, and resolution after removal.
Slit-lamp microscopy detects stromal thinning, ring protrusion, and epithelial defects. Fluorescein staining confirms epithelial defects. Corneal topography identifies unstable ring position.
CAS-OCT (corneal anterior segment OCT) is useful for assessing extrusion risk. It is performed at the first week and first month after ICRS implantation, and cases with an average depth percentage less than 60% or tunnel depth less than 70% are considered high risk.
Anterior stromal necrosis is a finding that precedes extrusion by about one year. It involves stromal thinning and ring exposure, with staining after cotton-tip debridement. An inflammatory halo may appear around the tunnel. Stromal infiltration suggests possible infection.
Explanation is the definitive treatment for ICRS extrusion. Indications include extrusion, decreased or fluctuating visual quality, corneal melting, infectious keratitis, contact lens intolerance, and corneal perforation.
There are two incision methods depending on the situation. If the extrusion is near the incision site, use a sinskey hook to open the previous entry. If the incision site has healed, create an incision window under the extruded ring with a diamond knife set to the original depth. In either case, close the defect with 10-0 nylon sutures.
When Complicated by Infectious Keratitis
Culture testing: Perform cultures from conjunctival and corneal scrapings in all cases.
Treatment: Combine high-concentration antibiotic eye drops with explantation. Antibiotics alone without explantation may also be effective in some cases.
Severe cases: In rapidly progressing cases, endophthalmitis may develop, requiring systemic antibiotics. Early full-thickness corneal transplantation may be an alternative.
Postoperative Management
Eye drops: Use antibiotic-steroid combination eye drops for 5 days.
Artificial tears: Use for 1–3 months, and instruct the patient to avoid rubbing the eye.
Adjunctive therapy: Promote epithelial healing with amniotic membrane transplantation or bandage contact lenses. In infected cases, continue high-concentration antibiotics at low frequency for 3 weeks after explantation.
In a report by Clinch et al., no worsening of corrected visual acuity, astigmatism, or myopia was observed after ring explantation. Traces of lamellar opacity decrease over time. Persistent incision scars do not cause visual impairment. Rarely, partial stromal melting, permanent stromal opacity, or corneal leukoma may remain.
QWill vision recover after explantation?
A
After explantation, epithelial defects resolve, and in most cases, visual acuity generally returns to approximately the preoperative level. Worsening of corrected visual acuity, astigmatism, or myopia is usually not observed. However, if permanent stromal opacity remains, visual recovery may be limited. Follow-up includes slit-lamp examination, visual acuity, and topography at 1 day, 1 month, 3 months, 6 months, and 1 year postoperatively.
The pathophysiology of ICRS extrusion is broadly divided into two mechanisms: ring migration and corneal melting.
Ring migration results from shallow implantation. When the ICRS is placed too shallow, anterior tensile strain increases, leading to stromal compression. Progression of compression in the anterior stromal depth causes epithelial and stromal breakdown, leading to corneal thinning and eventual spontaneous extrusion.
Corneal melting reflects an underlying inflammatory process. Kugler et al. proposed that surgical trauma during incision and tunnel creation induces progressive keratocyte apoptosis and tissue degeneration, resulting in corneal melting.
This progressive corneal melting is suggested to involve matrix metalloproteinases (MMPs). Introduction of exogenous stimuli or tear film insufficiency leads to overexpression of MMP-1 and MMP-2, causing degradation and thinning of the corneal matrix. In keratoconus itself, increased MMPs and decreased TIMP have been observed1), and IL-6, TNF-α, and MMP-9 in tears induce keratocyte apoptosis1).
QHow often does ICRS extrusion occur?
A
The exact incidence of ICRS extrusion varies among reports, but 48.2% of cases requiring ICRS removal are due to extrusion. The average onset time is about 10 years, ranging from 1 month to 20 years postoperatively. It has been reported that the extrusion rate significantly decreased after applying the pachymetry rule.
For prevention of ICRS extrusion, the usefulness of tunnel creation with femtosecond laser is attracting attention. Femtosecond laser provides precise tunnel dimensions, with advantages of minimal epithelial changes and faster recovery. However, some reports indicate no significant difference in extrusion rates compared to mechanical dissection, and a consensus has not been reached.
CAS-OCT has been proposed for early postoperative risk stratification. This approach identifies cases with an average depth percentage of less than 60% at the first week and first month after implantation, allowing close follow-up to prevent extrusion.
Superior segment placement has been reported to be effective in reducing progressive stromal thinning. Optimization of ring placement and adherence to the “pachymetry rule” are expected to further reduce extrusion rates.
For corneal reconstruction after ICRS extrusion, long-term outcomes of amniotic membrane transplantation (glycerin-preserved) have been reported, maintaining transparency up to 2 years. However, preventing myopic shift and increased astigmatism remains difficult, and further improvements are desired.
Jhanji V, Ahmad S, Amescua G, et al. Corneal Ectasia Preferred Practice Pattern. Ophthalmology. 2024 Apr;131(4):P205-P246. doi:10.1016/j.ophtha.2023.12.038. PMID:38349299.
Tlaiss Y, Warrak J, Warrak E. Intrastromal corneal ring segments for keratoconus: a comprehensive review of different types. Ther Adv Ophthalmol. 2025;17:25158414251371521. PMID: 40977849.
Monteiro T, Alfonso JF, Freitas R, Franqueira N, Faria-Correira F, Ambrósio R, et al. Comparison of Complication Rates between Manual and Femtosecond Laser-Assisted Techniques for Intrastromal Corneal Ring Segments Implantation in Keratoconus. Curr Eye Res. 2019;44(12):1291-1298. PMID: 31226888.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.