Complications arising in the lens capsule after cataract surgery are broadly classified into three types based on the behavior of lens epithelial cells (LECs). This article provides a comprehensive overview of these three conditions.
Condition
Abbreviation
Main mechanism
LEC status
Anterior capsule contraction syndrome
ACCS
Excessive contraction and fibrosis of the CCC opening
Excessive proliferation
Capsular block syndrome
CBDS
Fluid accumulation between the IOL and posterior capsule
Metaplasia and proliferation (late type)
Dead bag syndrome
—
Loss of structural support of the capsule and late IOL dislocation
Anterior Capsular Contraction Syndrome (ACCS) is a complication that occurs after phacoemulsification and intraocular lens (IOL) implantation. It refers to excessive contraction and fibrosis of the anterior capsular opening created by continuous curvilinear capsulorhexis (CCC).
First reported by Davison in 1993 1). Also called Capsule Contraction Syndrome (CCS) or anterior capsular phimosis.
According to ESCRS guidelines, the postoperative incidence is 0.47–3.3% 2), but some reviews report 1.4–14% 1), with onset most common within 3–30 weeks after surgery. Slight contraction of the opening is normal even in eyes without pathological changes, and contraction of about 10–20% usually does not cause clinical problems. However, excessive contraction progresses in eyes with specific risk factors.
Capsular Bag Distension Syndrome (CBDS) is a complication in which the capsular bag becomes sealed due to adhesion between the anterior surface of the IOL optic and the anterior capsule edge, leading to fluid accumulation between the IOL and the posterior capsule and distension of the posterior capsule. Also called capsular block syndrome (CBS). First reported by Davison in 1990 10).
The incidence is estimated at about 0.73% 6), and onset has been reported from a few weeks to 33 years after surgery 6). Based on Miyake et al.’s classification 5, 7), it is divided into three types: intraoperative (high irrigation pressure during hydrodissection), early postoperative (residual viscoelastic material), and late postoperative (metaplasia and proliferation of residual lens epithelial cells).
Dead Bag Syndrome is a condition in which all lens epithelial cells disappear after cataract surgery, resulting in the capsule being unable to hold the IOL on the optical axis. First named and reported by Dr. Samuel Masket. The capsule remains clear and thin but loses structural support, leading to late IOL dislocation9). The incidence of IOL malposition is reported as 0.2–3%, and the onset of late dislocation ranges from 4.5 to 16 years after surgery 9).
QHow often does anterior capsular contraction syndrome occur?
A
The postoperative incidence varies by study but is reported to be about 0.47–3.3%. It occurs more frequently in eyes with risk factors such as zonular weakness or pseudoexfoliation syndrome.
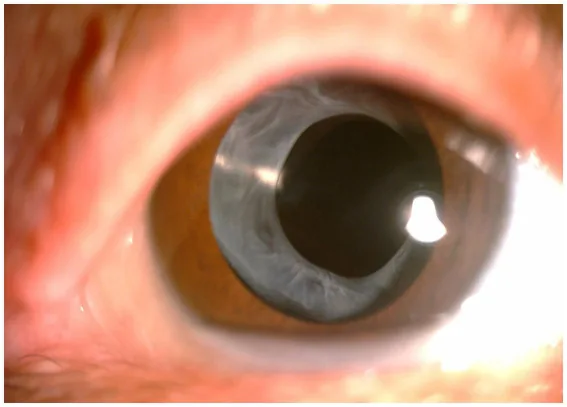
Lin X, et al. Exploring anterion capsular contraction syndrome in cataract surgery: insights into pathogenesis, clinical course, influencing factors, and intervention approaches. Front Med (Lausanne). 2024. Figure 1. PMCID: PMC10911763. License: CC BY.
Anterior segment photograph of a post-cataract surgery eye, showing the anterior capsulotomy edge fibrosed to a gray-white color and the opening concentrically reduced. Radial folds of the anterior capsule are also seen, specifically illustrating the clinical findings of anterior capsule contraction syndrome.
Symptoms and Findings of Anterior Capsule Contraction Syndrome
Monocular diplopia: May occur with IOL displacement.
Sudden severe vision loss: Occurs when IOL dislocation happens. Rarely, it may lead to ciliary body detachment or retinal detachment3).
Refractive changes: Capsular contraction causes IOL displacement or deformation, resulting in myopic or hyperopic shift. Some degree of myopic shift has been reported in 42% of patients 1).
Observation of the CCC opening with a slit-lamp microscope is fundamental.
Mild to Moderate
Reduction of the opening: The created CCC window visibly shrinks and often becomes non-circular.
Fibrous thickening: White opaque tissue forms along the anterior capsule edge.
Fold formation: Radial folds (wrinkles) are observed in the anterior capsule.
Severe
Complete occlusion of the opening: The visual axis is completely blocked. Fibrous plaque fills the opening.
IOL decentration/tilt: The IOL becomes decentered or tilted due to a decrease in the capsular equator diameter.
IOL dislocation: The IOL dislocates together with the capsule due to excessive traction on the zonules.
If postoperative blurred vision, decreased visual acuity, or impaired pupillary function is observed, actively check for signs of ACCS. Mydriatic examination allows more accurate assessment of the degree of opening deformation and fibrous opacity.
The main symptoms of CBDS are gradual visual decline, blurred vision, and myopic shift, often without eye pain. Slit-lamp examination typically reveals turbid fluid accumulation between the IOL and the posterior capsule.
Early Postoperative Type
Anterior IOL displacement: The IOL shifts forward due to posterior capsule distension.
Soemmering ring: May be observed as an accumulation of residual cortex and epithelial cells.
Normal intraocular pressure and anterior chamber depth: Often not accompanied by elevated intraocular pressure or shallow anterior chamber.
According to Vlasenko’s classification, CBDS is classified into four types: type 1 (clear capsule and clear fluid), type 2 (homogeneous milky fluid), type 3 (fluid accumulation with posterior capsule opacification), and type 4 (opaque contents with posterior capsule opacification). In the late stage, hidden endophthalmitis caused by Propionibacterium acnes (P. acnes) may be present, requiring attention7).
The main symptom is painless progressive vision loss, and refractive error worsens as the IOL gradually shifts9). Onset occurs several to more than ten years after cataract surgery.
Slit-lamp examination reveals the following characteristic findings:
IOL subluxation/dislocation: The IOL is displaced within the capsule, with inferior subluxation reported9).
Clear and thin lens capsule: The capsule is expanded, thin, and diaphanous9).
Absence of fibrosis and opacification: Both the anterior and posterior capsules are clear, with no signs of anterior capsule contraction or posterior capsule opacification9).
Floppy bag: Loss of capsular tone with flaccid folds9).
Case reports suggest that IOL support becomes unstable in a clear, thinned capsule9).
QIf vision decreases after cataract surgery, which capsular complication should be suspected?
A
Posterior capsule opacification (PCO) is the most common cause, but other conditions to differentiate include anterior capsule contraction syndrome (contraction and fibrosis of the anterior capsule), capsular block syndrome (fluid accumulation behind the IOL), and dead bag syndrome (IOL displacement in a clear capsule). In addition to slit-lamp examination, anterior segment OCT and UBM are useful for differentiation.
The material and design of the IOL affect the incidence of ACCS.
Silicone and hydrophilic acrylic IOLs have a higher incidence of ACCS compared to hydrophobic acrylic IOLs3, 4). Hydrophobic acrylic IOLs adhere strongly to the posterior capsule, inhibiting LEC proliferation and migration1).
Plate-haptic design IOLs carry a risk of IOL deformation (“double arch” deformation) that induces ACCS compared to loop-haptic IOLs4).
A 360° continuous square-edge design tends to reduce the incidence of ACCS3).
CBDS occurs through different mechanisms depending on the time of onset. Intraoperative type is caused by high perfusion pressure during hydrodissection, early postoperative type is mainly due to incomplete removal of ophthalmic viscosurgical devices (OVD) from the capsule, and late postoperative type is primarily driven by metaplasia and proliferation of residual lens epithelial cells and osmotic gradients5, 6, 7).
The following risk factors have been identified:
Small anterior capsulotomy (CCC diameter ≤5 mm): A small CCC that completely covers the IOL optic is the greatest risk factor7).
High myopia with axial length >25 mm: Increased risk confirmed in large retrospective studies.
Four-haptic IOL: Higher risk compared to C-loop IOLs.
Residual cortical material: Believed to be involved in almost all cases6).
The diagnosis of ACCS in post-cataract surgery patients is based on the presence of anterior capsule contraction confirmed by slit-lamp microscopy. It may or may not be accompanied by a decrease in best-corrected visual acuity compared to postoperative levels.
Examination Method
Purpose
Slit-lamp examination
Evaluate the shape, size, and fibrosis of the CCC opening
Dilated examination
Assess overall opening deformation and IOL displacement
Suspect CBDS in patients complaining of decreased vision after cataract surgery (regardless of postoperative duration). Slit-lamp examination confirms turbid fluid accumulation between the IOL and posterior capsule. Anterior segment OCT is useful for quantitative assessment of IOL displacement, and UBM is superior in cases of marked distention or when the posterior capsule is not visible 5, 6, 7).
Differential diagnoses include ordinary posterior capsule opacification (opacification of the posterior capsule adherent to the posterior surface of the IOL without fluid space), chronic endophthalmitis due to P. acnes, and pupillary blockglaucoma.
Slit-lamp examination confirms IOL displacement along with a clear, thin, and lax capsular bag, and absence of fibrosis or opacification 9). Differentiation from pseudoexfoliation syndrome (with residual lens epithelial cells and fibrotic changes) and true exfoliation syndrome (with lamellar peeling of the capsule) is important. If the capsule is removed, histological confirmation of complete absence of lens epithelial cells and lamellar peeling of the capsule at the zonular attachment site is performed 9).
The first-line treatment for mild to moderate ACCS is Nd:YAG laser anterior capsulotomy (relaxing incision), which can be performed easily on an outpatient basis.
Key points of the procedure are as follows.
Set the laser to anterior focus.
Adjust the energy to 1–3 mJ.
Make 4–6 radial nicks on the fibrotic anterior capsule edge.
Treatment guideline: Perform before phimosis progresses and the opening diameter becomes less than 4 mm.
Note that circular excision (removing the annular capsular tissue) is not recommended because the excised fragments may deposit in the angle and cause elevated intraocular pressure.
To prevent intraocular pressure elevation, instill apraclonidine hydrochloride (Iopidine) 1 hour before and immediately after the procedure.
Recent studies report that the ring YAG laser method (ring YAG) has a significantly higher capsular bag relaxation rate (94.4% vs 66.7%) and better safety than conventional radial incision methods1). There are also reports of femtosecond laser-assisted capsulotomy for the treatment of capsular contraction1).
This is an invasive surgery indicated for cases with severe fibrosis causing marked capsular thickening and significant IOL decentration. After incising the capsule with capsular scissors, a tearing maneuver is performed with forceps1).
Xu et al. reported that CBRS performed in 25 CCS patients resulted in significant improvement in postoperative visual acuity compared to preoperative values1).
This is indicated for severe cases with dense fibrous plaques where Nd:YAG laser and vitrectorhexis are ineffective. Bimanual dissection and peeling of the fibrous membrane using 23-gauge trocars have been reported, achieving visual axis clearance and visual recovery3).
The first-line treatment for CBDS is Nd:YAG laser posterior capsulotomy, which is also described in the AAO Cataract in the Adult Eye PPP (2021) 8). An incision is made in the posterior capsule to drain the accumulated fluid into the vitreous cavity, restoring the IOL to its original position. The prognosis is excellent; the cloudy fluid disappears after a few laser shots, and vision quickly returns to baseline.
The treatment strategy by type according to the Vlasenko classification is as follows.
When the posterior capsule is invisible due to cloudy fluid, treatment with conventional Nd:YAG laser is difficult. Posterior capsulotomy using a femtosecond laser with intraoperative OCT has been reported as an option for severe late-stage CBDS at the case report level 5).
When the posterior capsule is invisible or endophthalmitis due to P. acnes is suspected, a surgical approach combining PPV and posterior capsulotomy is selected. In cases of late CBDS or infection, reports have described vitrectomy combined with posterior capsule management6, 7).
Remove IOL-capsule complex and insert secondary IOL
For IOL subluxation within the capsule due to dead bag syndrome, IOL repositioning has been reported 9). If capsular damage is severe or the IOL itself is problematic, the IOL-capsule complex is removed and a secondary IOL is inserted.
QIs Nd:YAG laser treatment painful? Will I need to undergo it multiple times?
A
Nd:YAG laser is a painless outpatient procedure that takes a few minutes. In most cases, a single treatment is effective, and recurrence is rare. However, if fibrosis is severe, multiple sessions or surgery may be required.
6. Pathophysiology and detailed mechanism of onset
The core of ACCS pathophysiology is the proliferation and fibrotic metaplasia of lens epithelial cells (LECs) remaining in the capsule after surgery 1, 3).
When LECs are stimulated by surgical trauma, they produce fibrosis-promoting cytokines such as TGF-β, FGF, interleukin-1, and interleukin-6 1). These cytokines alter the microenvironment of the aqueous humor, causing LECs to secrete collagen fibers.
LECs undergo epithelial-mesenchymal transition (EMT) and differentiate into myofibroblasts 1, 3). Myofibroblasts express α-smooth muscle actin (α-SMA) filaments and proliferate and extend from the CCC edge onto the IOL surface. This process generates two complementary mechanisms of anterior capsule contraction.
Centripetal contraction of the capsulotomy window (purse-string contraction)
Occlusion of the residual opening by formation of a fibrous membrane
TGF-β acts as a “master regulator” of EMT, and after cataract surgery, disruption of the blood-aqueous barrier activates TGF-β1). The TGF-β/Smad pathway is involved in the pathogenesis of both ACCS and posterior capsule opacification (PCO). Smad7 protein is attracting attention as an EMT suppressor1).
When anterior capsule contraction occurs, an imbalance between the centripetal force from the anterior capsule edge and the centrifugal force from the zonules is important3). In eyes with weak zonules, the centripetal force dominates, making contraction and fibrosis more pronounced. In high myopia, the concentration of TGF-β2 in the aqueous humor increases, promoting the transformation of LECs into myofibroblasts4).
MMP-2 plays an important role in TGF-β2-mediated matrix contraction and posterior capsule opacification. Inhibition of MMP-2 is being studied as a novel therapeutic strategy for ACCS and PCO1).
The core of the pathophysiology of late-onset CBDS involves two mechanisms: metaplasia and proliferation of residual LECs, and osmotic gradient5, 6, 7).
Metaplasia and proliferation pathway: Residual LECs at the equator undergo fibroblast-like metaplasia and begin to proliferate. LECs produce extracellular matrix such as collagen type IV, and the residual cortex swells and liquefies, leading to accumulation of a milky white turbid fluid within the capsule (called lacteocrumenasia)7). Analysis of the fluid from treated cases has detected large amounts of α-crystallin by electrophoresis.
Osmotic gradient pathway: The osmotic gradient between the hyperosmolar contents inside the capsule and the hypoosmolar aqueous humor promotes fluid influx, accelerating capsular distension6).
Early postoperative type is caused by the sealing effect of residual OVD due to its high viscosity and high osmolarity, while intraoperative type results from excessive distension of the posterior capsule due to high-pressure injection during hydrodissection.
In dead bag syndrome, contrary to ACCS, LECs are completely absent, so no postoperative cellular responses (PCO, anterior capsule contraction) occur9).
Loss of capsular structural maintenance function: LECs directly interact with the capsular basement membrane and produce protective factors such as SPARC (secreted protein) to maintain capsular integrity. When LECs are lost, the capsule becomes thin and degenerates9).
Lamellar delamination of the capsule at the zonular attachment site: In a histological study of 10 cases by Culp et al., capsules lacking LEC showed lamellar delamination centered at the zonular attachment, leading to loss of zonular fibers and dislocation of the capsule-IOL complex 9).
Lack of contractile force: Normally, the contractile force of myofibroblasts maintains capsular tension, but in dead bag syndrome this is absent, causing the capsule to relax.
QWhy do some people develop anterior capsule contraction syndrome after cataract surgery while others do not?
A
The main reason is the presence or absence of risk factors. In eyes with pseudoexfoliation syndrome, diabetes, high myopia, or uveitis, LEC are more easily activated and zonules are fragile, making the balance between centripetal and centrifugal forces prone to disruption. Additionally, the material and design of the IOL used affect the incidence rate. Interestingly, when LEC are completely absent, it leads to the contrasting complication of dead bag syndrome.
Intraoperative 360° anterior capsule polishing may reduce LEC adhesion to the capsule and suppress postoperative capsular deformation. One report found that the anterior capsule opening area was larger in the polished group compared to the non-polished group at 12 months 1). However, the effect on posterior capsule opacification (PCO) is inconsistent across studies, and no definitive conclusion has been reached at this time 1).
Aspirin has been shown to potentially suppress the EMT process of LEC. In a human lens capsule model, the EMT inhibitory effect was enhanced in an aspirin concentration-dependent manner 1). Application to IOL-mounted drug delivery systems is being considered.
Resveratrol may suppress TGF-β2-induced fibrosis-related gene expression and reduce LEC proliferation on the posterior capsule. It has been shown to inhibit capsular wrinkling and is attracting attention as a future candidate for preventing PCO and ACCS 1).
G-CSF (granulocyte colony-stimulating factor) has been reported to promote proliferation, migration, EMT, and extracellular matrix synthesis in human lens epithelial cells (HLEC-B3). Regulation of G-CSF expression may be a target for PCO treatment 1).
Insertion of a capsular tension ring (CTR) in eyes with weak zonules has been reported to prevent postoperative IOL decentration and tilt, as well as to suppress anterior capsule contraction 4).
Antibiofouling IOLs that suppress LEC adhesion, photodynamic inhibition IOLs for LECs, and micropattern surface IOLs are under development, and are expected to be applied to prevent capsular opacification and contraction in the future 1).
Expanding Application of Femtosecond Laser to CBDS
Femtosecond lasers have been used for anterior capsulotomy, nuclear fragmentation, and corneal incisions in cataract surgery, but their application to CBDS is a relatively new attempt 5). Intraoperative OCT-guided femtosecond laser posterior capsulotomy has been reported as a candidate for severe late-stage CBDS where conventional Nd:YAG laser is not applicable. Equipment cost and access issues are limiting factors 5).
Elucidation of the Pathogenesis of Dead Bag Syndrome
The exact pathogenesis of dead bag syndrome remains unknown, and elucidating the molecular mechanisms leading to LEC loss is a future challenge 9). Some case reports suggest an association with systemic conditions, but at present this remains hypothetical 9). Studies are needed on the optimal extent of capsular polishing and the balance between LEC preservation and prevention of posterior capsule opacification.
Lan P, Nie L, Zhao L. Anterior Capsular Contraction Syndrome in Cataract Surgery: A Review of Challenges and Solutions. Medical science monitor : international medical journal of experimental and clinical research. 2025;31:e949046. doi:10.12659/MSM.949046. PMID:40936232; PMCID:PMC12439513.
Hartman M, Rauser M, Brucks M, Chalam KV. Evaluation of anterior capsular contraction syndrome after cataract surgery with commonly used intraocular lenses. Clin Ophthalmol. 2018;12:1399-403. [ESCRS Cataract Guideline掲載データより]
Guedes-Mota C, Dutra-Medeiros M, Tavares Ferreira J, Dias-Santos A. Surgical approach for management of complete anterior capsular contraction syndrome. BMJ case reports. 2024;17(1). doi:10.1136/bcr-2023-257851. PMID:38191223; PMCID:PMC10806895.
Wang W, Xu D, Liu X, Xu W. Case series: “Double arch” changes caused by capsule contraction syndrome after cataract surgery in highly myopic eyes. BMC ophthalmology. 2021;21(1):367. doi:10.1186/s12886-021-02113-z. PMID:34663265; PMCID:PMC8522032.
Lim XH, Patil M, Mehta JS. Femtosecond laser-assisted posterior capsulotomy for the treatment of capsular block syndrome. Taiwan journal of ophthalmology. 2023;13(3):371-375. doi:10.4103/tjo.TJO-D-23-00042. PMID:38089506; PMCID:PMC10712758.
Lizzio RAU, Polimeni F, Dellavalle A, D’Ancona F, Colombo M, Mattioli S, Nucci P. Late-onset capsular bag distension syndrome 33 years after cataract surgery. Am J Ophthalmol Case Rep. 2024;36:102112. doi:10.1016/j.ajoc.2024.102112.
Al-Mulla AH, Al-Rushoud MW. Unusual Late Presentation of Capsular Bag Distension Syndrome Associated With Propionibacterium acnes Endophthalmitis. Cureus. 2021;13(11):e19684. doi:10.7759/cureus.19684.
American Academy of Ophthalmology Preferred Practice Pattern Cataract and Anterior Segment Committee. Cataract in the Adult Eye PPP. 2021.
Thakur A, Bansal M, Challa D, Malhotra C, Jain AK. Dead bag syndrome-in the capsular bag subluxated intraocular lens centration and refixation: A new technique. Indian J Ophthalmol. 2023;71(10):3412-3414. doi:10.4103/IJO.IJO_1061_23. PMID:37787245. PMCID:PMC10683701.
Davison JA. Capsular bag distension after endophacoemulsification and posterior chamber intraocular lens implantation. J Cataract Refract Surg. 1990;16(1):99-108. doi:10.1016/S0886-3350(13)80883-8.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.