Jason Ruck. Non-mydriatic Topcon retinal camera. Wikimedia Commons. 2007. Figure 1. Source ID: commons.wikimedia.org/wiki/File:Retinal_camera.jpg. License: CC BY-SA 3.0.
This is a photo of the appearance of a non-mydriatic fundus camera made by Topcon, showing the standard tabletop type with a main unit, eyepiece, chin rest, and control joystick. It corresponds to the non-mydriatic fundus camera device discussed in the section “1. What is non-mydriatic fundus photography?”
Non-mydriatic fundus photography is an imaging test that photographs the fundus without using dilating drops. In a dark room or a dimly lit room, it encourages the pupils to dilate naturally and observes the posterior pole with a coaxial illumination fundus camera using the indirect method. The standard field of view is 45°, and imaging focuses on the macula, optic disc, and areas around the vascular arcades.
In settings that combine a non-mydriatic wide-field fundus camera and OCT, it is possible to obtain wide-area, highly accurate diagnostic images even without dilation. Depending on the conditions, it may be better than ophthalmoscopic observation for detecting retinal hemorrhage. However, observing the most peripheral retinal findings requires a dilated fundus examination.
It is widely used for screening diabetic retinopathy, glaucoma, AMD, and hypertensive retinopathy. In recent years, combining it with AI (artificial intelligence) automatic analysis has attracted attention for improving screening efficiency1), and use of fundus photography in telemedicine (teleophthalmology) is also expanding2).
QWhat is a non-mydriatic camera?
A
It is a device that can photograph the fundus without using dilating drops (eye drops). Images are taken in a dark room after the pupils have naturally widened. It also does not require anesthetic eye drops, and one advantage is that you can go home and drive right after the examination. However, if the pupils do not open enough or if detailed observation of the peripheral back part of the eye is needed, an examination using dilating drops may be necessary.
Non-mydriatic fundus camera (standard type)
Field of view: 45° (imaging centered on the posterior pole)
Anesthesia: No anesthetic eye drops needed
Main imaging modes: color, green (red-free), infrared
Evaluation criteria: Further examination if the C/D ratio is 0.7 or higher, or if the difference between the eyes is 0.2 or greater. Further examination if the R/D ratio is 0.1 or lower
Note: Combine this with OCT measurement of retinal nerve fiber layer (RNFL) thickness
AI analysis: Deep learning has high accuracy for automatic detection of glaucomatous optic neuropathy5)
For screening in patients with diabetes, two posterior pole images (centered on the optic disc and macula) are standard. If a wide-angle camera is available, one image may be used instead. After non-mydriatic imaging, adding OCT to evaluate macular edema is recommended. If the stage has progressed to preproliferative or beyond, consider further examination with fluorescein angiography (FA).
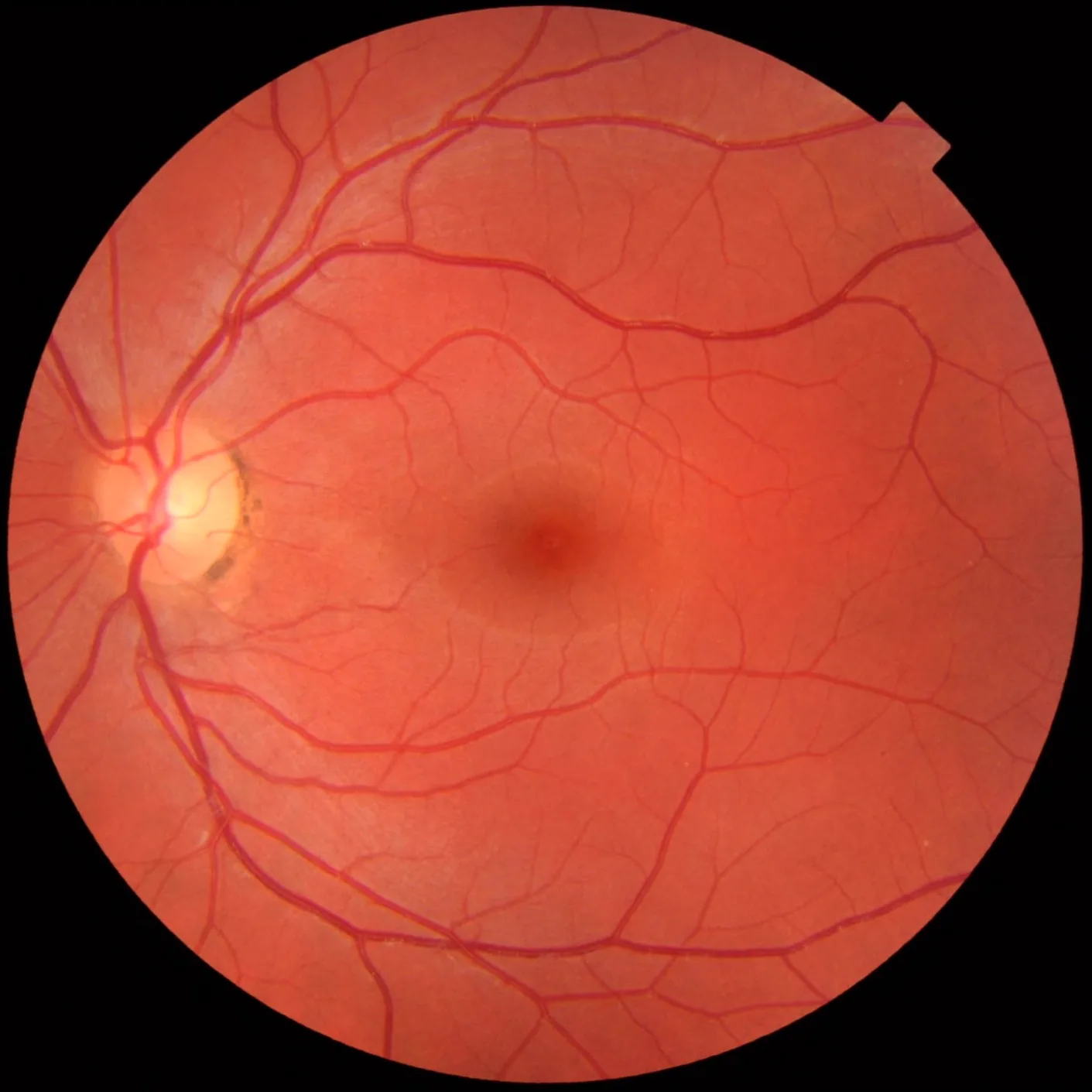
Mikael Haggstrom. Fundus photograph of normal left eye. Wikimedia Commons. 2012. Figure 1. Source ID: commons.wikimedia.org/wiki/File:Fundus_photograph_of_normal_left_eye.jpg. License: CC BY-SA.
This color fundus photograph of the left eye of a healthy 25-year-old man shows normal fundus findings, including a clear orange-red optic disc, macula, upper and lower vascular arcades, and the course of the retinal vessels. It corresponds to the normal optic disc and macular findings covered in section “4. How to read normal and abnormal findings.”
Peripheral retina cannot be observed: Non-mydriatic imaging mainly targets the posterior pole. Dilation is needed to observe lattice degeneration and retinal tears
Vitreous cannot be observed: If evaluation of vitreous opacity, such as in uveitis, is needed, dilated fundus examination is essential
Decreased quality with cataract and small pupils: If lens opacity is severe or the pupil does not dilate (small pupil), image quality decreases
Depends on pupil size: If the pupil does not dilate enough (guide: less than 4 mm), a clear image cannot be obtained
The use of mydriatic drops is determined based on the state of the anterior chamber angle and social factors at the visit, such as whether the patient will drive. Confirm the following before dilation.
Anterior chamber angle: Generally contraindicated if angle-closure glaucoma or suspected angle-closure glaucoma is present
Phenylephrine allergy: Checking the medical history is essential, especially at the first dilation
Driving cars or bicycles: Do not drive for 4 to 6 hours after dilation. Explain this to the patient beforehand
Types of dilation drops: A mixed eye drop of tropicamide (0.5–1%) and phenylephrine (2.5–5%) is commonly used
QIs it okay not to dilate the pupils?
A
In routine follow-up exams for stable diabetes and glaucoma, combining a wide-field fundus camera with OCT is often enough without pupil dilation. However, if detailed observation of inflammation inside the eye (uveitis) or the peripheral retina is needed, or at the first visit, a dilated exam is recommended. After dilation, vision becomes blurry for about 4 to 6 hours, but this is temporary.
A non-mydriatic fundus camera is a coaxial-illumination fundus camera (indirect method). It observes the retina through the cornea, lens, and vitreous. It consists of the following components.
Light source: The retina is illuminated with a flash lamp (white, green, blue, infrared)
Imaging sensor: Images are captured digitally with a CCD or CMOS sensor
Optical system: An objective lens, field lens, and fundus lens form an inverted real image
Spectral filters: Swapped according to the imaging mode (color, green, infrared, FAF, etc.)
Color photography: The most commonly used. Allows overall assessment of hemorrhage, white spots, and optic disc shape
Green light (red-free) photography: Removes red light and highlights the superficial nerve fiber layer and hemorrhages. Useful for observing NFLD
Infrared photography: Used to observe deeper layers (retinal pigment epithelium and choroid). Less affected by cataracts and vitreous opacities
Fundus autofluorescence (FAF): Detects lipofuscin fluorescence using short-wavelength blue light (488 nm) excitation. Evaluates the metabolic state of the retinal pigment epithelium. Useful for assessing AMD, retinitis pigmentosa, and geographic atrophy
Save as digital images in the electronic medical record and use them for comparison of changes over time. A standard resolution of 15 megapixels or higher is recommended. Record the imaging date, eye, imaging direction, and camera settings.
Automatic AI diagnosis of diabetic retinopathy: Research is progressing on detecting diabetic retinopathy with high sensitivity and specificity through automatic analysis of fundus images using deep learning. AI diagnostic systems developed and validated with data from multiethnic populations have been reported1). In addition, a pivotal trial of an autonomous AI diagnostic system in primary care has been conducted, and efforts toward practical use are accelerating4)
Use in teleophthalmology: Teleophthalmology, in which images taken with a non-mydriatic fundus camera are interpreted remotely by ophthalmology specialists, is becoming more widespread. It is contributing especially to diabetic retinopathy screening in areas where access to ophthalmologists is difficult2). However, issues remain with image quality assurance, system setup, and reimbursement
Glaucoma AI screening: Research is also progressing on automatic detection of glaucomatous optic neuropathy using deep learning on color fundus photographs. One study reported performance comparable to specialists5)
UK Diabetic Retinopathy Screening Programme: National non-mydriatic fundus camera screening has been carried out since 2003 and has helped reduce vision loss from diabetes3)
Ting DSW, Cheung CY, Lim G, Tan GSW, Quang ND, Gan A, et al. Development and Validation of a Deep Learning System for Diabetic Retinopathy and Related Eye Diseases Using Retinal Images From Multiethnic Populations With Diabetes. JAMA. 2017;318(22):2211-2223. doi:10.1001/jama.2017.18152. PMID:29234807; PMCID:PMC5820739.
Sim DA, Keane PA, Tufail A, et al. Automated retinal image analysis for diabetic retinopathy in telemedicine: potential and pitfalls. Ophthalmic Surg Lasers Imaging Retina. 2015;46(6):615-624.
Scanlon PH. The English National Screening Programme for diabetic retinopathy 2003-2016. Acta Diabetol. 2017;54(6):515-525.
Abràmoff MD, Lavin PT, Birch M, Shah N, Folk JC. Pivotal trial of an autonomous AI-based diagnostic system for detection of diabetic retinopathy in primary care offices. NPJ digital medicine. 2018;1:39. doi:10.1038/s41746-018-0040-6. PMID:31304320; PMCID:PMC6550188.
Li Z, He Y, Keel S, et al. Efficacy of a deep learning system for detecting glaucomatous optic neuropathy based on color fundus photographs. Ophthalmology. 2018;125(8):1199-1206.