
IHAPSH (Intrapapillary Hemorrhage with Adjacent Peripapillary Subretinal Hemorrhage)
Key Points at a Glance
Section titled “Key Points at a Glance”1. 視神経乳頭出血(IHAPSH)とは
Section titled “1. 視神経乳頭出血(IHAPSH)とは”Intrapapillary Hemorrhage with Adjacent Peripapillary Subretinal Hemorrhage(IHAPSH)は、視神経乳頭内(intrapapillary)の出血と、それに連続する乳頭周囲網膜下(peripapillary subretinal)の出血を同時に認める臨床像を指す。視神経乳頭浮腫様の所見を伴うこともあり、若年・近視眼に好発する良性の症候群として位置づけられる1)。
乳頭出血と乳頭周囲網膜下出血を同一眼に認める病態は、1975年のCibisらによる後部硝子体剥離に伴う網膜出血の報告にさかのぼる2)。1995年にはKatzとHoytが、若年者で後部硝子体剥離が不完全な状態で生じる乳頭内・乳頭周囲出血を硝子体乳頭牽引(vitreopapillary traction)の所見として報告した3)。2004年、Kokameらが9例(女性7例・男性2例、平均年齢47歳、屈折は−1.00〜−9.50D)について「intrapapillary hemorrhage with adjacent peripapillary subretinal hemorrhage」として独立した症候群を提唱し、現在の名称が定着した1)。
Epidemiology
Section titled “Epidemiology”The exact incidence is unknown, but case reports in Japan tend to be biased toward young, myopic women. In the initial 9 cases reported by Kokame et al., the majority were women, and refractive errors ranged from mild to high myopia 1). Bilateral cases are relatively rare, but there are reports of sequential onset in both eyes over a 2-year course in a 25-year-old woman 5) and similar findings in both eyes at a 2-month interval in a 36-year-old woman 6). Cases in teenagers are also increasing, with typical examples accumulating in an 11-year-old girl 7), a 12-year-old 9,10), a 17-year-old 11), and a 19-year-old 1).
The nationwide incidence is not known. Most reports are case-based, indicating it is clearly a rare condition. However, it is noted that it may be more common in populations with overlapping young age, myopia, and posterior vitreous detachment, and the actual frequency might be somewhat higher than recognized.
2. Main Symptoms and Clinical Findings
Section titled “2. Main Symptoms and Clinical Findings”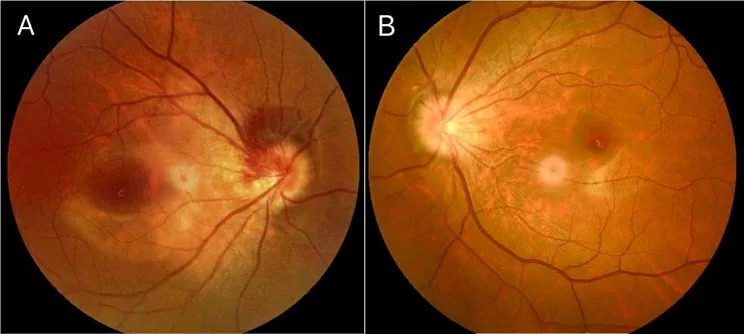
Subjective Symptoms
Section titled “Subjective Symptoms”Typical subjective symptoms are floaters and mild blurred vision. Many cases are asymptomatic and discovered incidentally during routine eye exams or workup for other diseases. Visual acuity is often well preserved; in Kokame et al.’s initial 9 cases, 7 maintained visual acuity of 1.0 or better 1). In Japanese cases, a 12-year-old girl with corrected visual acuity of 0.9/1.2 at initial visit 10), a 17-year-old maintaining 1.2 in both eyes 11), and an 11-year-old girl with 1.2/1.2 7) have been reported.
However, when hemorrhage extends into the vitreous cavity or involves subretinal hemorrhage near the macula, blurred vision, visual field defects, and central scotoma may occur. A case of a 62-year-old woman with vitreous hemorrhage and peripapillary subretinal hemorrhage resulting in a corrected visual acuity of 0.01 in the right eye has been reported 4).
Fundus Findings
Section titled “Fundus Findings”Three characteristic hemorrhagic components are observed simultaneously or sequentially 1,4).
- Intrapapillary hemorrhage: Red to dark red hemorrhage spreading radially on the optic disc surface.
- Peripapillary subretinal hemorrhage: Pale red to dark red hemorrhage extending from the disc margin to the nasal to inferonasal side, with less distinct borders than intraretinal hemorrhage.
- Vitreous hemorrhage: In mild cases, appears as thin hemorrhagic floaters in front of the disc; in severe cases, it may obscure fundus examination.
Peripapillary subretinal hemorrhage often occurs on the nasal side4,7,8,10), which is thought to be related to the small scleral canal of the optic disc and the direction of vitreous traction. At onset, it may be accompanied by mild disc edema-like swelling, requiring differentiation from papilledema9). Hwang and Lin summarized multilayered optic disc hemorrhages in adolescents, showing that three-layer hemorrhages (disc surface, subretinal, and vitreous) represent a continuous pathology explained by the same mechanism21).
Visual Field Findings
Section titled “Visual Field Findings”Visual field changes are mild, presenting as enlargement of the Mariotte blind spot or Bjerrum scotoma, and are often asymptomatic. Goldmann or Humphrey perimetry may show arcuate sensitivity loss or nasal step corresponding to the hemorrhage site. After hemorrhage resolution, visual field defects usually improve1,5).
Course and Prognosis
Section titled “Course and Prognosis”In principle, hemorrhage is naturally absorbed over a course of 6 weeks to several months without treatment. In Kokame et al.’s observation, 7 out of 9 cases recovered visual acuity of 1.2 or better, and no recurrence was observed 1). In typical cases in Japan, there are reports of a 12-year-old girl whose vitreous hemorrhage disappeared 6 weeks after the first visit and corrected visual acuity improved to 1.0 10), and a 36-year-old woman with bilateral involvement who recovered to 1.2 in the right eye and 1.0 in the left eye after 2 months 6). Recurrence is rare, but there are cases where onset occurs at different times in both eyes, so follow-up of the contralateral eye is necessary even after unilateral onset 5,6).
3. Causes and Risk Factors
Section titled “3. Causes and Risk Factors”Related Anatomical Factors
Section titled “Related Anatomical Factors”- Small optic disc and small scleral canal: Teng et al. reported that crowded optic nerve head and small scleral canal are associated with IHAPSH 13). Dense nerve fibers within the disc and a small scleral canal opening may predispose to hemorrhage with minor mechanical stress.
- Disc tilt: Takahashi et al. used swept-source OCT to show that the disc tilt angle in IHAPSH eyes is larger than in control eyes 14). A case in Japan with tilted disc syndrome, PHOMS, and IHAPSH also supports the association between tilt and this condition 15).
- Myopia and axial elongation: Most reported cases involve mild to high myopia, and there is a case of a 12-year-old girl who developed the condition during the progression of myopia 9). Axial elongation and weakening of peripapillary tissue are thought to be underlying factors.
- Association with PHOMS (peripapillary hyperreflective ovoid mass-like structures): PHOMS are ovoid hyperreflective structures observed on Bruch’s membrane around the optic disc and are thought to reflect axoplasmic flow stasis 16,17). Several Japanese reports have described PHOMS in patients with IHAPSH 15,18), suggesting common anatomical and mechanical predispositions. In children, PHOMS have been reported as a frequent cause of pseudopapilledema 22), and the prevalence of PHOMS is significantly higher in children with myopia 23).
Related mechanical factors
Section titled “Related mechanical factors”- Posterior vitreous detachment (PVD) and vitreopapillary traction: Cibis et al. reported that PVD can cause optic disc hemorrhage and retinal hemorrhage 2), and Katz and Hoyt showed that vitreopapillary traction due to incomplete PVD can cause optic disc hemorrhage in young individuals 3). In a 62-year-old Japanese case, PVD and rupture of superficial optic disc vessels were suspected as the bleeding mechanism 4).
- Valsalva-like blood pressure fluctuations: Severe coughing, defecation, exercise, and other causes of sudden venous pressure elevation may trigger bleeding 12).
Patient background as a risk factor
Section titled “Patient background as a risk factor”- Young women (10s to 30s)
- Myopia (mild to high)
- Tilted disc, small scleral canal, PHOMS
- Incomplete PVD, vitreopapillary adhesion
- Strong eye movements or Valsalva maneuver
4. Diagnosis and Examination Methods
Section titled “4. Diagnosis and Examination Methods”Basics of Diagnosis
Section titled “Basics of Diagnosis”The starting point for diagnosis is the ophthalmoscopic confirmation of “intrapapillary hemorrhage” and “adjacent peripapillary subretinal hemorrhage” in the same eye. When findings such as nasally displaced subretinal hemorrhage, mild vitreous hemorrhage, and a background of young age, myopia, or female sex are present, IHAPSH should be strongly suspected 1,4).
Imaging Tests
Section titled “Imaging Tests”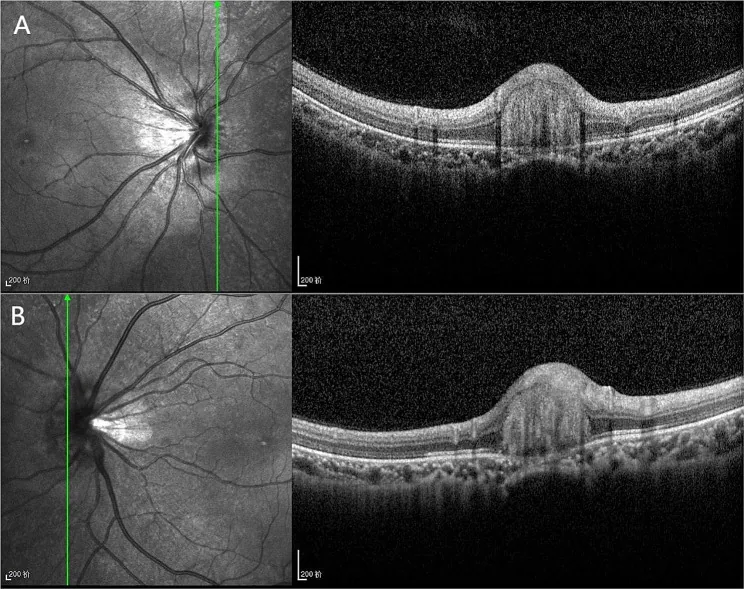
- Optical coherence tomography (OCT): Evaluates the layered structure of intrapapillary and peripapillary hemorrhage. Hemorrhage is captured as a hyperreflective image extending into the subretinal space, and the presence of PHOMS (oval hyperreflective lesions above the Bruch’s membrane opening) is also confirmed10,15,16). Swept-source OCT is useful for observing optic disc tilt angle, small scleral canal, and PHOMS14,15).
- OCT angiography (OCTA): Used to rule out choroidal neovascularization (CNV) and evaluate flow signals within PHOMS. In isolated IHAPSH, CNV is generally not observed10,11).
- Fluorescein angiography (FA) / Indocyanine green angiography (IA): Evaluates the presence of CNV and dye leakage from the optic disc. In this condition, only fluorescence blockage at the hemorrhage site is observed, with no active CNV1,12).
- 頭部MRI/MRA/MRV:うっ血乳頭・特発性頭蓋内圧亢進症(IIH)の鑑別に必要である。本邦の30代IIH 例では empty sella と PHOMS を認め、髄液圧 300 mmH₂O が確認された19)。IHAPSH 単独例では中枢神経画像に異常を認めない。
視野・電気生理検査
Section titled “視野・電気生理検査”Goldmann 視野・Humphrey 視野で Mariotte 盲点の拡大や Bjerrum 型暗点の有無を評価する。本症単独では中心視野は保たれることが多い。視神経炎を疑う場合には visual evoked potential(VEP)や色覚検査を併用する。
| 鑑別疾患 | 鑑別のポイント |
|---|---|
| Non-arteritic anterior ischemic optic neuropathy (NAION) | Elderly, acute vision loss with severe visual field defect, mainly optic disc edema |
| Optic neuritis | Pain on eye movement, central scotoma, relative afferent pupillary defect (RAPD) |
| Glaucomatous optic neuropathy | Chronic course, characteristic optic disc cupping and RNFL defect |
| Congestive optic disc / IIH | Bilateral papilledema, headache, pulsatile tinnitus, elevated CSF pressure |
| Optic disc drusen | Autofluorescence, OCT, ultrasound for calcification assessment |
| Tilted disc syndrome alone | Congenital optic disc dysplasia without hemorrhage |
| Terson syndrome | Preceded by central nervous system events such as subarachnoid hemorrhage |
| Traumatic optic disc hemorrhage | Clear history of trauma |
| Papillary hemorrhage related to blood disorders | Systemic findings such as severe anemia and thrombocytopenia20) |
5. Standard Treatment
Section titled “5. Standard Treatment”Observation as a Principle
Section titled “Observation as a Principle”IHAPSH is a benign disease that resolves spontaneously, and no definitive drug therapy or surgical treatment has been established. Many reports indicate that bleeding subsides within 6 weeks to a few months with observation alone 1,6,10,11).
Key Points for Observation
Section titled “Key Points for Observation”- Initial evaluation: Combine visual acuity, refractive correction, intraocular pressure, visual field, OCT, and FA/OCTA to rule out CNV, optic neuritis, and papilledema.
- Observation interval: Initially every 1–2 weeks; once a reduction in bleeding is confirmed, extend to every 1–2 months. When visual acuity is stable, transition to regular checkups every 6 months.
- Lifestyle guidance: Advise avoiding strong straining or Valsalva maneuvers. It is safer to refrain from contact sports and extreme eye movements in the short term.
- Evaluation of the fellow eye: Given the possibility of bilateral onset, even in unilateral cases, OCT and visual field of the fellow eye should be assessed over time5,6).
Exceptional interventions
Section titled “Exceptional interventions”Only when CNV is present or when bleeding extends to the macula and persistently affects visual function, anti-VEGF therapy or vitrectomy may be considered on a case-by-case basis. There is insufficient evidence to support the use of antithrombotic drugs or corticosteroids for this condition alone. In cases with persistent visual field defects or vision loss, reassess for concomitant chronic optic neuropathy or overlooked other diseases.
6. Pathophysiology and Detailed Mechanism of Onset
Section titled “6. Pathophysiology and Detailed Mechanism of Onset”Mechanical Traction Hypothesis
Section titled “Mechanical Traction Hypothesis”The most supported mechanism is that nerve fibers and blood vessels densely packed in a small scleral canal of the optic disc are mechanically damaged by vitreopapillary traction associated with incomplete posterior vitreous detachment (PVD), leading to rupture of superficial capillaries1,3,13). Hemorrhage can spread simultaneously into three layers: the optic disc surface, peripapillary subretinal space, and vitreous cavity.
Vascular and Tissue Vulnerability
Section titled “Vascular and Tissue Vulnerability”In myopic axial elongation and tilted disc syndrome, distortion of the scleral canal morphology, thinning of the peripapillary choroid, and enlargement of the Bruch’s membrane opening occur, making the tissue vulnerable to vitreous traction and intraocular pressure fluctuations14,15). In a Japanese case of combined tilted disc syndrome, PHOMS, and IHAPSH, it was suggested that the anatomical predisposition of the tilted disc promoted both PHOMS and IHAPSH15).
Association with PHOMS
Section titled “Association with PHOMS”PHOMS are ovoid hyperreflective structures observed above the Bruch’s membrane opening on OCT. Initially, differentiation from optic disc drusen was a concern, but they are now understood to reflect axoplasmic flow stasis of retinal nerve fibers 16,17). Borrelli et al. demonstrated blood flow signals within PHOMS on OCTA 17). Tokuhisa et al. reported bilateral PHOMS in a 12-year-old girl with IHAPSH, suggesting that the coexistence of PHOMS and IHAPSH may not be coincidental 18). Yamamoto et al. also presented an 11-year-old case with tilted disc syndrome accompanied by PHOMS and IHAPSH, discussing the possibility that PHOMS may predispose to the development of IHAPSH 15).
Hemodynamic factors
Section titled “Hemodynamic factors”Sudden venous pressure elevation similar to Valsalva maneuver, vigorous eye movements, and blood pressure fluctuations during exercise are thought to promote rupture of mechanically weakened superficial optic disc vessels 12). Many cases have described an association between this condition and episodes of physical exertion or straining before onset.
Integrated model
Section titled “Integrated model”In summary, IHAPSH can be understood as a multifactorial hemorrhage resulting from the combination of (1) anatomical predisposition of the optic disc (small scleral canal, tilted disc, PHOMS, myopia), (2) vitreopapillary traction (incomplete PVD), and (3) transient hemodynamic stress. After onset, traction is relieved as PVD progresses, and the hemorrhage is naturally absorbed 1,3,13,14).
7. Latest Research and Future Prospects
Section titled “7. Latest Research and Future Prospects”Advances in Imaging Diagnostics
Section titled “Advances in Imaging Diagnostics”The widespread use of swept-source OCT and OCTA has made it possible in routine clinical practice to evaluate PHOMS, optic disc tilt, and three-dimensional understanding of the Bruch membrane opening 14,17). Takahashi et al. quantified the large optic disc tilt in IHAPSH eyes 14), and small case series in Japan have repeatedly shown a high rate of coexistence of tilted disc and PHOMS 15,18).
Refinement of Disease Characteristics through Case Accumulation
Section titled “Refinement of Disease Characteristics through Case Accumulation”Multiple case reports suggest a tendency for onset clustering in young women (teens) and middle-aged women (30s–40s), but the limited number of cases has not led to a definitive onset pattern 7,9,10,11). Accumulation of bilateral cases and late-onset recurrences has also progressed, reaffirming the importance of surveillance of the fellow eye after unilateral onset 5,6).
Development of a Differential Diagnosis Algorithm
Section titled “Development of a Differential Diagnosis Algorithm”Since PHOMS is also observed in IIH and demyelinating diseases, it is necessary to carefully rule out the coexistence of IIH or optic neuritis in IHAPSH with PHOMS. A Japanese case report of IIH with PHOMS in a 30-year-old patient highlights the importance of systematic evaluation when PHOMS findings are detected 19). In the future, an algorithm that parameterizes the presence, size, and distribution of PHOMS to quantify the risk of developing IHAPSH is expected.
Prevention and Patient Education
Section titled “Prevention and Patient Education”Although clear preventive measures have not been established, controlling myopia progression, appropriate refractive correction, and avoiding strong Valsalva maneuvers may theoretically reduce mechanical stress on the optic disc. The intersection with management strategies for childhood myopia is a future challenge 9).
8. References
Section titled “8. References”- Kokame GT, Yamamoto I, Kishi S, et al. Intrapapillary hemorrhage with adjacent peripapillary subretinal hemorrhage. Ophthalmology. 2004;111(5):926-930. doi:10.1016/j.ophtha.2003.08.040.
- Cibis GW, Watzke RC, Chua J. Retinal hemorrhages in posterior vitreous detachment. Am J Ophthalmol. 1975;80(6):1043-1046. doi:10.1016/0002-9394(75)90334-7.
- Katz B, Hoyt WF. Intrapapillary and peripapillary hemorrhage in young patients with incomplete posterior vitreous detachment. Signs of vitreopapillary traction. Ophthalmology. 1995;102(2):349-354. doi:10.1016/s0161-6420(95)31018-4.
- 牧野伸二, 武澤美喜子, 久保田美由紀, ほか. 硝子体出血と乳頭周囲網膜下出血を伴った傾斜乳頭症候群の1例. 臨床眼科. 2005;59(3):277-281.
- 西智, 湯川英一, 松浦豊明, ほか. 両眼に発症したIntrapapillary Hemorrhage with Adjacent Peripapillary Subretinal Hemorrhage(IHAPSH)の1例. あたらしい眼科. 2009;26(6):845-847.
- 坂井公彦, 春田雅俊, 石橋由美, ほか. 両眼に発症したintrapapillary hemorrhage with adjacent peripapillary subretinal hemorrhageの1例. 臨床眼科. 2020;74(3):335-339.
- 永岡光輔, 月井利佳, 渡邉芽里, ほか. 11歳女児にみられたintrapapillary hemorrhage with adjacent peripapillary subretinal hemorrhageの1例. 眼科. 2021;63(4):381-385.
- 田辺智子, 森富彦, 江口修一郎. 17歳に発症した典型的なintrapapillary hemorrhage with adjacent peripapillary subretinal hemorrhage(IHAPSH)の1例. 眼科. 2020;62(12):1363-1366.
- 高橋恭一. 近視進行期に発症したintrapapillary hemorrhage with adjacent peripapillary subretinal hemorrhage(IHAPSH)の1例. 臨床眼科. 2022;76(2):241-244.
- 町田葵, 寺崎浩人, 三原直久, ほか. 若年で発症したintrapapillary hemorrhage with adjacent peripapillary subretinal hemorrhage(IHAPSH)の1例. 臨床眼科. 2024;78(4):431-436.
- Caryssa L. Yan, Marten E. Brelen, Haoyu Chen, Weiqi Chen. Spontaneous intrapapillary hemorrhage with adjacent peripapillary subretinal hemorrhage in adolescents. cleverjournal. 2019;2(1):6-10. doi:10.15713/ins.clever.21.
- Moon IH, Lee SC, Kim M. Intrapapillary hemorrhage with concurrent peripapillary and vitreous hemorrhage in two healthy young patients. BMC ophthalmology. 2018;18(1):172. doi:10.1186/s12886-018-0833-z. PMID:30005697; PMCID:PMC6045832.
- Teng Y, Yu X, Teng Y, Xu B, Sun Q, Dong L, et al. Evaluation of crowded optic nerve head and small scleral canal in intrapapillary hemorrhage with adjacent peripapillary subretinal hemorrhage. Graefe’s archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2014;252(2):241-8. doi:10.1007/s00417-013-2459-4. PMID:24057175.
- Takahashi S, Kawashima R, Morimoto T, Sakimoto S, Shiozaki D, Nishida K, et al. Analysis of optic disc tilt angle in intrapapillary hemorrhage adjacent to peripapillary subretinal hemorrhage using swept-source optical coherence tomography. American journal of ophthalmology case reports. 2022;27:101598. doi:10.1016/j.ajoc.2022.101598. PMID:35651596; PMCID:PMC9149012.
- 山本大輔, 永岡光輔, 牧野伸二, ほか. PHOMSとIHAPSHがみられた傾斜乳頭症候群の1例. 眼科. 2024;66(12):1513-1519.
- Fraser JA, Sibony PA, Petzold A, Thaung C, Hamann S, ODDS Consortium. Peripapillary Hyper-reflective Ovoid Mass-like Structure (PHOMS): An Optical Coherence Tomography Marker of Axoplasmic Stasis in the Optic Nerve Head. Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society. 2021;41(4):431-441. doi:10.1097/WNO.0000000000001203. PMID:33630781; PMCID:PMC9258618.
- Borrelli E, Barboni P, Battista M, Sacconi R, Querques L, Cascavilla ML, et al. Peripapillary hyperreflective ovoid mass-like structures (PHOMS): OCTA may reveal new findings. Eye (London, England). 2021;35(2):528-531. doi:10.1038/s41433-020-0890-4. PMID:32346103; PMCID:PMC7997888.
- 徳久輝明, 林孝彰, 西嶋怜美, ほか. 視神経乳頭出血を合併したperipapillary hyperreflective ovoid mass-like structures(PHOMS)の1例. 日本眼科学会雑誌. 2022;126(7):642-650.
- 岩井誠真, 粕谷由佳, 牧野伸二, ほか. 特発性頭蓋内圧亢進症に伴ったperipapillary hyperreflective ovoid mass-like structuresの1例. 眼科. 2025;67(9):827-836.
- Janetos TM, Bhasin A. Optic Disc Hemorrhages in Severe Anemia and Thrombocytopenia. Journal of general internal medicine. 2023;38(1):234-235. doi:10.1007/s11606-022-07853-2. PMID:36326990; PMCID:PMC9849492.
- Hwang JF, Lin CJ. Multilayered optic disk hemorrhages in adolescents. J Pediatr Ophthalmol Strabismus. 2014;51(5):313-318.
- Mezad-Koursh D, Klein A, Rosenblatt A, Teper Roth S, Neudorfer M, Loewenstein A, et al. Peripapillary hyperreflective ovoid mass-like structures-a novel entity as frequent cause of pseudopapilloedema in children. Eye (London, England). 2021;35(4):1228-1234. doi:10.1038/s41433-020-1067-x. PMID:32616868; PMCID:PMC8115042.
- Lyu IJ, Park KA, Oh SY. Association between myopia and peripapillary hyperreflective ovoid mass-like structures in children. Scientific reports. 2020;10(1):2238. doi:10.1038/s41598-020-58829-3. PMID:32041993; PMCID:PMC7010819.