Corneal epithelial stem cells reside in the limbus, where they differentiate and proliferate into basal epithelial cells while migrating centripetally, then move to the surface 1). In LSCD, these stem cells are damaged, and the corneal epithelium is replaced by conjunctival epithelium. This results in loss of corneal transparency and decreased vision 1). Corneal transplantation alone cannot reconstruct the ocular surface in LSCD, leading to epithelial healing failure and graft failure 2). Limbal stem cell transplantation (LSCT) can restore normal epithelial phenotype and achieve a stable corneal surface 2).
For unilateral LSCD, autograft from the healthy eye (CLAu) is possible, but bilateral LSCD requires allograft. CLAL has better histocompatibility and surgical outcomes compared to KLAL (from cadaveric donors) 3). Since Kenyon and Rapoza reported the first lr-CLAL in 1995, the procedure has evolved with improvements in donor selection protocols.
lr-CLAL is a method of transplanting limbal and conjunctival tissue from a living relative, while KLAL transplants corneal limbal tissue from a cadaveric donor. lr-CLAL has higher histocompatibility and lower graft rejection rates. Additionally, lr-CLAL can provide fresh conjunctiva simultaneously, making it more suitable for LSCD cases with conjunctival disease. On the other hand, KLAL is chosen when no compatible living relative is available.
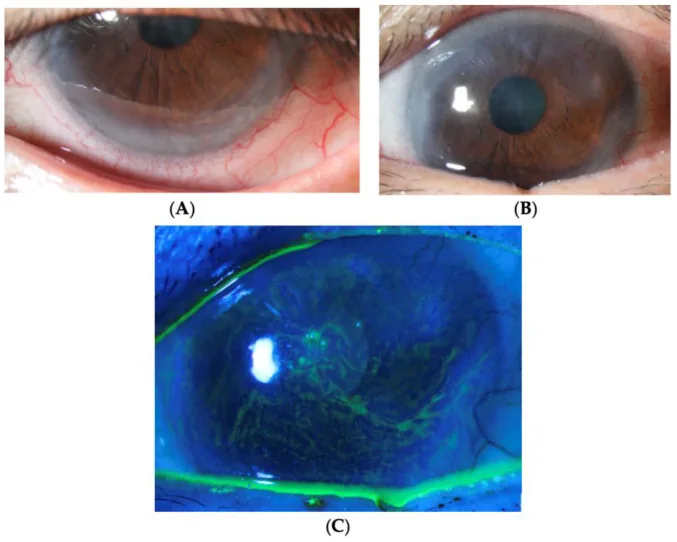
Yhu Fhei Lee, Dayna Wei Wei Yong, Ray Manotosh A Review of Contact Lens-Induced Limbal Stem Cell Deficiency 2023 Dec 5 Biology (Basel). 2023 Dec 5; 12(12):1490 Figure 2. PMCID: PMC10740976. License: CC BY.
A and B show conjunctival invasion, neovascularization, and pannus extending from the corneal periphery to the center. C shows punctate staining along the whorl-like epithelium on fluorescein staining, indicating epithelial instability.
Patients with LSCD who are candidates for lr-CLAL complain of eye pain, photophobia, tearing, and decreased vision 3). Visual impairment worsens as conjunctivalization progresses. In unilateral cases, decreased vision on the affected side is the main complaint.
Whorl-like epitheliopathy: A whorl-like pattern of epithelial damage is seen on fluorescein staining. This is an early finding of mild LSCD1).
Loss of palisades of Vogt (POV): The palisade structure of the limbus disappears. This is a basis for clinical diagnosis of LSCD.
Conjunctivalization: The corneal epithelium is replaced by conjunctival epithelium. It can be confirmed by the appearance of goblet cells on the cornea1).
Corneal neovascularization: Superficial neovascularization and pannus appear from moderate stage onward 1).
Severity Classification
Partial LSCD: A part of the cornea is conjunctivalized. Limbal stem cells remain 1).
Total LSCD: The entire corneal surface is conjunctivalized. Limbal stem cells are completely lost 1).
Staging by the Limbal Stem Cell Working Group: Stage 1 (central 5 mm clear), Stage 2 (central 5 mm involved), Stage 3 (entire corneal surface involved) 3).
Subclassification by limbal involvement: A (≤50%), B (>50% to <100%), C (100%) are further subdivided3)
In a single-center study of 738 eyes, aniridia accounted for 30.9%, chemical/thermal injury for 20.6%, contact lens-related for 16.8%, and SJS for 10.4%1). In unilateral LSCD, chemical injury is the most common cause1).
Other reported causes include glaucoma surgery (with mitomycin C/5-FU)1), radiation exposure1), infectious keratitis1), and vernal keratoconjunctivitis1).
Relative contraindications for lr-CLAL include significant conjunctival inflammation/scarring, marked mucin deficiency, aqueous tear deficiency, and ocular surface keratinization. These conditions are associated with poor OSST prognosis. Medical contraindications to systemic immunosuppression are also relative contraindications.
In impression cytology, the presence of conjunctival goblet cells indicates conjunctivalization1). Immunohistochemical staining for cytokeratin 3 (corneal epithelial marker) and cytokeratin 19 (conjunctival epithelial marker) is used for differentiation1).
Donor selection is extremely important for the success of lr-CLAL. The Cincinnati donor selection protocol evaluates candidates through the following steps.
Identify first-degree relative candidates
Perform ABO blood typing
Perform panel reactive antibody (PRA) and donor-specific antibody (DSA) testing
Perform HLA typing and virtual crossmatch
Perform serological testing for HIV, hepatitis, and cytomegalovirus
Perform detailed examination of the donor eye to rule out subtle stem cell deficiency
QWhat kind of person is suitable as a donor?
A
The ideal donor is a first-degree relative with compatible ABO blood type and high HLA compatibility. The donor eye must have no history of long-term contact lens wear, no prior ocular surgery, and no ocular surface disease. According to the Cincinnati protocol, blood type, antibody testing, HLA typing, and infectious disease screening are performed stepwise to select the most suitable donor.
lr-CLAL surgery is performed in two stages: harvesting of donor segments and transplantation into the recipient eye.
Donor segment harvesting: Conjunctival and limbal segments of approximately 2 clock hours each are harvested from the 12 o’clock and 6 o’clock positions. The total harvested amount should be less than 6 clock hours to prevent inducing LSCD in the donor eye. The conjunctiva is elevated with BSS injection, and blunt dissection is performed 1 mm beyond the limbus onto the cornea to include stem cells.
Recipient eye preparation: A 360-degree conjunctival incision is made, and the conjunctiva is recessed 2–3 mm. The thickened Tenon’s capsule is excised, and abnormal corneal epithelium and fibrovascular pannus are removed. Amniotic membrane may be used concurrently to promote epithelialization and suppress inflammation.
Placement of donor tissue: The harvested segments are fixed at the 12 o’clock and 6 o’clock positions with 10-0 nylon sutures. The base is adhered to the sclera with tissue adhesive, and a large-diameter bandage contact lens is placed.
Concurrent surgeries may include scar dissection (most common), amniotic membrane transplantation, and penetrating keratoplasty3). Corneal transplantation after CLAL should be delayed for at least 12 months postoperatively due to inflammation risk 3).
Systemic immunosuppression is essential for long-term graft survival after lr-CLAL.
Cincinnati OSST Immunosuppression Protocol:
Tacrolimus 4 mg twice daily plus mycophenolate mofetil (MMF) 1 g twice daily, started 1–2 weeks before surgery
Prednisone 1 mg/kg/day added postoperatively, tapered over 1–3 months
Valganciclovir and TMP/SMX administered for 6 months to prevent opportunistic infections
After ocular surface stabilization, tacrolimus is tapered starting 12–18 months postoperatively, and MMF starting 3 years postoperatively. If there is a history of rejection, low-dose immunosuppression is continued indefinitely. Cyclosporine A and MMF have been reported to have good tolerability even with long-term use 3).
Postoperative topical treatment: Moxifloxacin 0.5%, loteprednol 1%, cyclosporine A 1% eye drops, and preservative-free artificial tears are used 3).
Combined OSST Procedure
Cincinnati method (KLAL/lr-CLAL): Indicated for bilateral cases with severe cicatricial conjunctival disease and total limbal deficiency. lr-CLAL segments are placed at 12 and 6 o’clock, and KLAL tissue is added at 3 and 9 o’clock to achieve nearly 360-degree limbal reconstruction.
lr-CLAL/CLAu combination: Indicated for severe unilateral LSCD with concurrent limbal and conjunctival disease. It minimizes antigen load while maximizing healthy limbal stem cells and conjunctival volume.
Complications and Management
Acute rejection: Occurs in 10–40% of cases. Presents with pain, hyperemia, graft swelling, and epithelial rejection line. Treated with increased topical and systemic steroids.
Chronic rejection: Leads to gradual surface failure and graft thinning. Increasing systemic immunosuppressants is effective.
Secondary glaucoma: May develop due to long-term steroid use or underlying disease 3). If topical treatment is ineffective, trabeculectomy or tube shunt surgery may be indicated 3).
QHow long is immunosuppression continued?
A
When the ocular surface is sufficiently stable, tacrolimus tapering begins 12–18 months postoperatively, and MMF tapering begins 3 years postoperatively. However, if there is a history of graft rejection, low-dose immunosuppression must be continued indefinitely. Management of immunosuppressants should be coordinated with organ transplant specialists, and regular blood tests are performed to monitor side effects.
QDoes the donor eye experience any effects?
A
By limiting the harvest from the donor eye to 2–2.5 clock hours per conjunctival/limbal segment and a total of less than 5 clock hours, the risk of inducing LSCD in the donor eye is considered low. Postoperatively, antibiotic eye drops are used for about one week. The possibility of serious complications in the donor eye is low, but thorough preoperative explanation and consent are necessary.
The essence of LSCD, the target disease of lr-CLAL, is the disruption of corneal epithelial homeostasis due to limbal stem cell dysfunction.
The corneal epithelium is a stratified squamous epithelium that continuously regenerates 1). The palisades of Vogt (POV), described by Vogt in 1921, are radial structures located at the limbus containing arterial and venous components 1). Limbal stem cells reside in the basal layer of the POV and function as a source of corneal epithelial regeneration 1).
When LSCD occurs, the corneal epithelium is replaced by conjunctival epithelium, and goblet cells appear on the cornea1). Conjunctivalization leads to loss of corneal transparency and decreased vision 2). If 7% of corneal stem cells remain, regeneration of corneal epithelium is possible with modern surgical techniques 1).
The therapeutic principle of lr-CLAL is that healthy limbal stem cells transplanted from a donor restore a normal epithelial phenotype on the recipient’s cornea2). The transplanted stem cells engraft in the limbus and regenerate the corneal epithelium while migrating centripetally. Since conjunctiva is also transplanted simultaneously in lr-CLAL, it compensates for conjunctival defects and supplies goblet cells.
The severity of the condition varies depending on the cause of LSCD. In chemical injuries, not only the limbus but also the conjunctiva and corneal stroma are extensively damaged, requiring more invasive treatment 3). In aniridia, congenital limbal stem cell dysfunction due to PAX6 gene mutation is the cause, leading to a chronic progressive course.
Kasikci et al. analyzed 19 eyes with CLAL and reported a success rate of 52.6% at 1 year postoperatively 3). The success rate was significantly higher in eyes with lower preoperative LSCD stage (p=0.04), and in chemical injury cases, longer intervals from injury to surgery were associated with better outcomes (p=0.001) 3). The severity of chemical injury showed a negative correlation with surgical success (p=0.001) 3). The degree of relatedness between donor and recipient (first-degree vs. second-degree) did not significantly affect the success rate 3).
In a systematic review by Shanbhag et al., the ocular surface stabilization rate at a mean follow-up of 2.9 years for CLET was 61.4% (357 of 581 eyes), and a BCVA improvement of 2 or more lines was observed in 51.5% (219 of 425 eyes) 2). Chemical injury accounted for 90% of LSCD causes 2).
Advances in LSCD diagnostic techniques: Anterior segment OCT is being studied as a non-contact diagnostic method for LSCD based on corneal epithelial thickness measurement 1). It offers advantages over impression cytology and confocal microscopy in terms of speed and minimal invasiveness 1).
Future challenges:
Prospective evaluation of long-term outcomes using the LSCD staging system 3)
Standardization and optimization of donor selection protocols
Optimization of immunosuppressive regimens and reduction of side effects
Hu JCW, Trief D. A narrative review of limbal stem cell deficiency & severe ocular surface disease. Ann Eye Sci. 2023;8:13.
Shanbhag SS, Nikpoor N, Rao Donthineni P, Singh V, Chodosh J, Basu S. Autologous limbal stem cell transplantation: a systematic review of clinical outcomes with different surgical techniques. The British journal of ophthalmology. 2020;104(2):247-253. doi:10.1136/bjophthalmol-2019-314081. PMID:31118185.
Kasikci M, Korkmaz I, Palamar M, Egrilmez S, Yagci A, Barut Selver O. Evaluation of the factors that influence surgical outcome in conjunctival-limbal allograft transplantation. Eye (London, England). 2023;37(11):2192-2196. doi:10.1038/s41433-022-02314-w. PMID:36418907; PMCID:PMC10366148.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.