Central bouquet abnormalities (CB abnormalities) are not an independent disease entity. They are a classification system for foveal microstructural changes observed on OCT associated with vitreoretinal interface diseases and cystoid macular edema (CME).
Central bouquet (CB) refers to a circular area approximately 100 μm in diameter at the center of the fovea. This region is composed of cone photoreceptors and Müller cells and is one of the most important structures for vision. The term “bouquet” originates from Rochon Duvigneaud’s initial description of the foveal cone arrangement, and Gass proposed the concept of the “Müller cell cone.” Govetto et al. later systematically studied CB abnormalities in tractional diseases 3).
CB abnormalities are defined as a progressive spectrum consisting of the following three stages:
Stage 1 (cotton ball sign): A small, poorly defined hyperreflective area appearing between the ellipsoid zone (EZ) and the interdigitation zone (IZ).
Stage 2 (foveal detachment): Subretinal fluid accumulation observed as a hyporeflective pocket beneath the IZ.
Stage 3 (acquired vitelliform lesion): Accumulation of dome-shaped, thick hyperreflective material formed between the EZ and the RPE.
QIs central bouquet abnormality a disease?
A
Central bouquet abnormality is not an independent disease. It is a classification system for foveal microstructural changes observed on OCT, appearing in association with underlying conditions such as epiretinal membrane, vitreomacular traction, and cystoid macular edema. Diagnosis and management of the underlying disease are essential.
There are no subjective symptoms specific to CB abnormalities. Symptoms due to the underlying disease (e.g., epiretinal membrane, vitreomacular traction, cystoid macular edema) are predominant.
Decreased visual acuity: Visual acuity tends to decrease as the CB stage progresses.
Diagnosis of CB abnormality is based on OCT. Findings for each stage are shown below.
Stage 1
Cotton ball sign: A small, poorly defined hyperreflective area appearing between the EZ (ellipsoid zone) and IZ (interdigitation zone).
EZ and ELM are preserved: In this stage, the continuity of the external limiting membrane (ELM) and ellipsoid zone is often maintained.
Visual acuity: Relatively well preserved.
Stage 2
Foveal detachment: Subretinal fluid observed as a hyporeflective pocket directly beneath the IZ. Indicates detachment of the cone and RPE.
Possible EZ disruption: Partial disruption of the EZ may occur in this stage.
Visual acuity: Moderate decrease.
Stage 3
Acquired vitelliform lesion: A dome-shaped thick hyperreflective material formed between the EZ and RPE. Indicates accumulation of metabolic products beneath the cone.
ELM disruption: Disruption of the ELM occurs in this stage.
Visual acuity: Often poor.
The OCT findings for each stage are summarized below.
When an epiretinal membrane (ERM) is the underlying condition, it is observed as a hyperreflective line on the internal limiting membrane (ILM). Some reports indicate that in stages 3–4 of epiretinal membrane staging, the incidence of CB abnormalities decreases with the formation of ectopic inner foveal layers (EIFL).
Epiretinal membrane is a fibroproliferative membrane formed on the internal limiting membrane of the retina, with aging being a major risk factor 1). Traction from the epiretinal membrane is transmitted to the foveal cones via Müller cells, causing CB abnormality.
In VMT, the vitreous remains adherent to the macula due to incomplete posterior vitreous detachment (PVD). In focal VMT (adhesion width approximately 500 μm), foveal elevation and cyst formation occur, while in broad VMT (adhesion width approximately 1500 μm), macular detachment may result 1). Perifoveal PVD leads to dissociation of Müller cell cones and photoreceptors, forming intraretinal cysts 2).
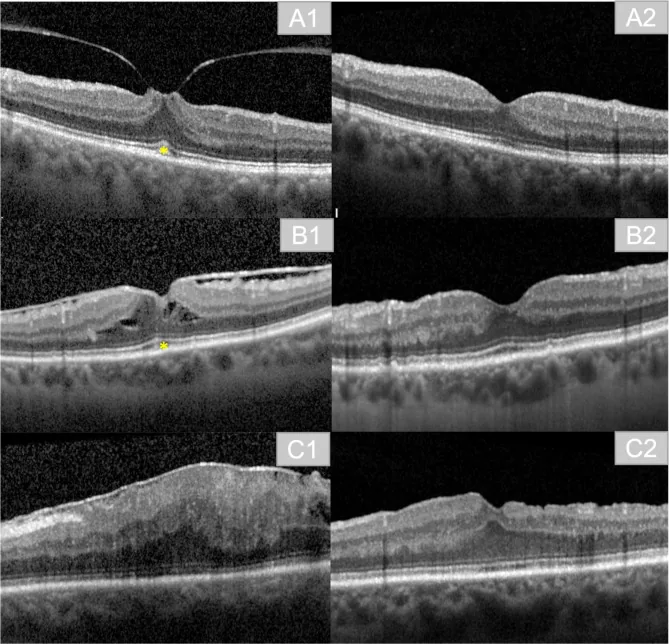
Verena Anna Englmaier; Jens Julian Storp; Nicole Eter; Sami Al-Nawaiseh. Short-term-outcomes of idiopathic epiretinal membranes treated with pars-plana-vitrectomy – examination of visual function and OCT-morphology. Int J Retina Vitreous. 2023 Sep 14; 9:55 Figure 2. PMCID: PMC10500920. License: CC BY.
Exemplary imaging of pre- and postoperative results. A1: preoperative finding in a patient with vitreomacular traction (VMT) and Cotton Ball sign (). A2: postoperative result in the same patient at three months postoperatively. B1: preoperative finding in a patient with ERM, Cotton Ball sign (), and intraretinal cavities due to ERM. B2: postoperative result in the same patient at three months postoperatively. C1: preoperative finding in a patient with ERM Stage 4. C2: postoperative result in the same patient at three months postoperatively
Diagnosis of CB abnormalities is made solely by OCT. No specific examination techniques or blood tests are required.
Optical coherence tomography (OCT) allows staging of microstructural changes in the CB. After understanding the findings of each stage (see the “Clinical findings” section), the diagnosis is made in conjunction with evaluation of the underlying disease.
Each stage of CB abnormalities, especially stage 3 (acquired vitelliform lesion), requires differentiation from the following diseases.
Krill disease
Acute RPE inflammation (Krill disease): A self-limiting disease with multiple small yellowish lesions around the fovea. It usually resolves spontaneously within 6 to 12 weeks.
Key differentiating point: Spontaneous resolution and absence of underlying diseases (such as epiretinal membrane or VMT) are key to differentiation.
Key differentiating point: OCT morphology of PED and identification of leakage points on fluorescein angiography are useful for differentiation.
Vitelliform Macular Dystrophy
Best disease (vitelliform macular dystrophy): A hereditary disease. Characterized by deposition of yolk-like material beneath the RPE.
Key differentiating point: Young age of onset, family history, EOG abnormalities (decreased Arden ratio), and genetic testing contribute to differentiation.
Diagnosis can be made by OCT alone. Special blood tests, staining, or angiography are not mandatory. OCT staging of foveal microstructural changes (EZ, IZ, ELM, RPE) and evaluation for underlying diseases (epiretinal membrane, VMT, cystoid macular edema, etc.) are used for diagnosis.
Intravitreal injection: Anti-VEGF drugs or steroids are used. It is indicated for cystoid macular edema secondary to diabetic macular edema, retinal vein occlusion, and uveitis.
Most epiretinal membranes follow a stable course, and few progress 1). Over a 5-year natural history, 29% progress, 26% improve, and 39% remain stable 1).
For VMT, observation or vitrectomy (PPV) is considered. If symptoms are mild, observation is preferred; if traction is strong and vision loss progresses, surgery is considered.
QIs surgery necessary for cotton ball sign (stage 1)?
A
The cotton ball sign alone does not necessarily require surgery. Goveto et al. observed that many cases are stable. It may resolve when traction on the underlying disease is released. Observation or treatment intervention is decided based on a comprehensive assessment of visual acuity, metamorphopsia, and progression of the underlying disease.
The foveal bouquet (CB) is located in the deepest part of the fovea, an area approximately 100 μm in diameter, and consists of cone photoreceptors responsible for vision and their supporting Müller cells. Müller cells span from the internal limiting membrane (ILM) to the external limiting membrane (ELM), maintaining the structural integrity of the retina. Studies by Gass and Yamada have shown that Müller cells are more vertically oriented in the center of the fovea. This anatomical characteristic is thought to make the CB vulnerable to mechanical stress.
Tractional forces are transmitted to cone photoreceptors via Müller cells. The mechanisms of each stage are as follows.
Stage 1 (cotton ball sign): The cone is displaced upward due to inward traction. The EZ and ELM are preserved at this stage.
Stage 2 (foveal detachment): When traction exceeds the adhesion between the cone and RPE, the cone and RPE detach, and subretinal fluid appears. A break in the EZ may occur.
Stage 3 (acquired vitelliform lesion): Persistent detachment leads to accumulation of cone metabolic products between the RPE and cone, forming a dome-shaped hyperreflective material. A break in the ELM occurs. The hyperreflective material may eventually migrate into the retina and spontaneously collapse, but breaks in the EZ and ELM often persist.
In cystoid macular edema, fluid accumulation causes physical stretching of Müller cells, leading to mechanical stress on the CB. Persistent stretching may progress to foveal detachment (stage 2).
7. Clinical significance, prognosis, and future perspectives
Stage 1 (cotton ball sign): In many cases, it remains stable under observation (Goveto). It may resolve when traction on the underlying disease is relieved.
Stage 2 (foveal detachment): It may improve with treatment of the underlying disease.
Stage 3 (acquired vitelliform lesion): Migration of hyperreflective material into the retina and spontaneous collapse may be observed. However, breaks in the EZ and ELM often persist after collapse, and visual recovery tends to be limited.
Opinions vary among reporters regarding CB abnormalities and visual outcomes after ERM surgery.
There is no consensus on CB abnormalities and visual outcomes after ERM surgery. Reports indicate that timely ERM surgery may lead to good visual recovery, while the presence of preoperative CB abnormalities may be a poor prognostic factor for postoperative visual outcomes.
It has been suggested that the higher the stage of CB abnormality preoperatively, the poorer the postoperative visual recovery may be. This underscores the clinical significance of early detection of CB abnormalities and timely treatment of the underlying disease.
The concept of CB abnormality is a relatively new classification born with the development of OCT technology, and future research is expected on the following points.
The impact of CB abnormality stage on surgical indication and timing
Natural course and treatment response of CB abnormality associated with non-tractional cystoid macular edema
Quantitative evaluation of CB microstructure using high-resolution OCT (SS-OCT, OCTA)
QIf the stage progresses, can vision recover?
A
In stage 3 (acquired vitelliform lesion), even if the hyperreflective material collapses, disruption of EZ and ELM often persists. Visual recovery tends to be limited, and opinions among researchers are divided regarding surgical outcomes. Addressing the underlying disease at an early stage is considered important for improving visual prognosis.
Flaxel CJ, Adelman RA, Bailey ST, Fawzi A, Lim JI, Vemulakonda GA, et al. Idiopathic Epiretinal Membrane and Vitreomacular Traction Preferred Practice Pattern®. Ophthalmology. 2020;127(2):P145-P183. doi:10.1016/j.ophtha.2019.09.022. PMID:31757497.
Royal College of Ophthalmologists. Clinical Guideline on Idiopathic Full Thickness Macular Holes. London: RCOphth; (draft).
Govetto A, Bhavsar KV, Virgili G, Gerber MJ, Freund KB, Curcio CA, et al. Tractional Abnormalities of the Central Foveal Bouquet in Epiretinal Membranes: Clinical Spectrum and Pathophysiological Perspectives. Am J Ophthalmol. 2017;184:167-180. PMID: 29106913.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.