Optic neuropathy after COVID-19 is a general term for optic nerve disorders that develop after SARS-CoV-2 infection. Two main types have been reported.
Ischemic optic neuropathy (ION): Acute vision loss due to interruption of blood supply to the optic nerve. It is classified into anterior (AION) and posterior (PION), with AION further divided into arteritic (A-AION) and non-arteritic (NA-AION).
Optic neuritis (ON): A disease in which inflammation damages the optic nerve, leading to visual dysfunction. Both papillitis and retrobulbar optic neuritis types have been reported.
In adults, non-arteritic anterior ischemic optic neuropathy and optic neuritis are the two most common acute optic neuropathies. Temporal associations with COVID-19 infection have been reported both during infection (concomitant) and after infection (days to weeks after recovery). The exact mechanism remains unknown, but inflammatory reactions, hypercoagulable states, hypoxia, and autoimmune responses are thought to be involved.
QCan optic neuropathy also occur after COVID-19 vaccination?
A
Cases of non-arteritic anterior ischemic optic neuropathy and ON have been reported after vaccination. It has also been suggested that the combination of infection and vaccination may enhance the immune response. For details, see the section “Latest Research and Future Prospects”.
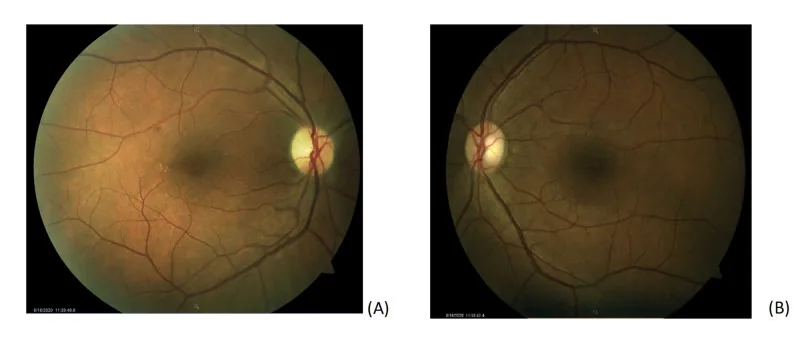
A Case of Non-Arteritic Anterior Ischemic Optic Neuropathy with COVID-19. Cureus.; 12(12):e11950. Figure 1. PMCID: PMC7785499. License: CC BY.
Color fundus photography of both eyes. (A) Fundus photo of the right eye showing a small microaneurysm with exudates along the superotemporal arcade without subretinal fluid and temporal pallor of the optic nerve. (B) Fundus photo of the left eye is normal with a cup-to-disk ratio of 0.3.
Orbital apex syndrome: Some cases are accompanied by eye movement pain and restriction.
QWhat is the difference in symptoms between ION and optic neuritis?
A
ION is characterized by painless acute vision loss, often noticed upon waking in the morning. In contrast, ON is accompanied by eye movement pain in about 60% of cases and is also more likely to involve color vision abnormalities. Visual field patterns also differ: ION often presents with horizontal hemianopia, while ON commonly shows central scotoma.
Structural factors: Small cup-to-disc ratio (disc at risk). Structural vulnerability of the optic nerve head.
Vascular factors: Diabetes, systemic hypertension, nocturnal hypotension, ischemic heart disease, anemia. COVID-19-related ION cases often have a history of diabetes and hypertension.
COVID-19-specific factors: Inflammatory cytokine release, hypercoagulable state, endothelial dysfunction, hypoxemia. These are thought to cause optic nerve ischemia via thrombosis of ciliary vessels.
Neurotropism: SARS-CoV-2 may cross the blood-brain barrier and enter the central nervous system via infected leukocytes.
Molecular mimicry: Viral antigens may trigger an autoimmune response against myelin proteins.
MOG-IgG antibodies: Cases have been reported where demyelination occurs through a MOGAD-like mechanism involving MOG antibody production.
Relationship with onset timing: There are both infection-associated (asymptomatic to mild illness) and post-infection (days to weeks after recovery) forms.
Visual acuity test and visual field test: Quantitative assessment using Humphrey visual field analyzer. Visual field patterns are useful for differentiating ION from ON.
Color vision test: ON shows color vision abnormalities such as red desaturation.
Pupillary light reflex test (RAPD): A finding strongly suggestive of optic nerve lesion.
Critical flicker frequency (CFF): Decreased in optic nerve diseases.
Fundus examination: Check for swelling, pallor, or hemorrhage of the optic disc.
Orbital MRI: In optic neuritis, contrast enhancement of the optic nerve and high signal on STIR images are observed. Fat-suppressed contrast-enhanced T1-weighted coronal images are useful. For evaluation of multiple sclerosis, check for periventricular demyelinating plaques on FLAIR images.
Fluorescein angiography (FAG): In AION, delayed filling of the optic disc is observed in the acute phase.
ESR/CRP: Measured to rule out giant cell arteritis. In giant cell arteritis, ESR/CRP levels are elevated in over 80% of cases, and CRP is more specific than ESR. However, note that COVID-19 itself increases inflammatory markers, making differentiation from giant cell arteritis difficult.
Anti-AQP4 antibody: Measured to differentiate steroid-resistant optic neuritis.
Anti-MOG antibody: Measured when a MOGAD-like mechanism is suspected.
Platelet count: Measured to evaluate coagulation abnormalities.
As criteria for atypical optic neuritis, if any of the following are met, diseases other than optic neuritis should be considered.
Age outside 15–45 years
Bilateral simultaneous onset
Progression beyond 2 weeks after onset
Steroid dependence
Presence of systemic symptoms
In differentiating non-arteritic anterior ischemic optic neuropathy from A-AION, temporal artery biopsy is important, especially in elderly patients. The sensitivity and specificity of temporal artery biopsy are both reported to be over 95%.
QCan elevated inflammatory markers in COVID-19 be mistaken for giant cell arteritis?
A
It is possible. In COVID-19 infection, ESR and CRP can be markedly elevated, which may be mistaken for findings of giant cell arteritis. Especially when AION occurs in elderly COVID-19 patients, careful evaluation including clinical symptoms and temporal artery biopsy is necessary, keeping in mind the incidental coexistence of giant cell arteritis.
Methylprednisolone 1,000 mg/day intravenous infusion for 3 days.
If no effect after the first course, administer a second course after an interval of 4–5 days.
After pulse therapy, start oral prednisolone at 0.5 mg/kg/day and taper by 5–10 mg every 3–4 days.
In COVID-19-related ON cases, the same pulse therapy plus oral tapering protocol is used, and with appropriate treatment, the prognosis is generally good. In idiopathic optic neuritis, even without treatment, visual improvement begins within 3 weeks of onset in about 80% of cases, and visual recovery is expected in over 90%.
In pediatric cases, adjust the dose based on body weight (methylprednisolone 15 mg/kg/day for 3 days, then taper oral prednisolone at 1 mg/kg).
Currently, there is no established effective treatment. Anticoagulation therapy, vasodilators, oral steroids, and optic nerve sheath decompression have been attempted, but no significant improvement in visual prognosis has been proven.
Management of underlying diseases: Control of arteriosclerotic risk factors including blood pressure and diabetes is important.
Thrombosis prevention: Antiplatelet therapy such as aspirin may be recommended.
Natural prognosis: Approximately 40% of patients with non-arteritic anterior ischemic optic neuropathy not associated with COVID-19 experience some spontaneous visual recovery. Papilledema resolves 1–2 months after onset, followed by slow progression of optic atrophy and pallor. Further vision loss after the stable phase is very rare.
Once a diagnosis is confirmed or strongly suspected, steroid therapy should be initiated promptly. Delayed treatment carries a high risk of involvement of the fellow eye (approximately 50% within days to weeks if untreated).
Intravenous therapy: Methylprednisolone 1 g/day for 3–5 days.
Oral taper: Start with prednisolone 1 mg/kg/day, then slowly taper over at least 4–6 months based on systemic condition and ESR levels. Some cases may require more than 1 year.
Prognosis: Visual improvement in the affected eye is rarely expected, but it is effective in preventing onset in the fellow eye. Only 4% experience visual function improvement with steroids.
Alternate-day steroid administration is not recommended.
QIs there no effective treatment for non-arteritic anterior ischemic optic neuropathy?
A
Currently, there is no established effective treatment. Management focuses on controlling arteriosclerosis risk factors (blood pressure, blood glucose) and preventing onset in the fellow eye. The annual incidence rate in the fellow eye is about 15–20%, making regular follow-up important.
6. Pathophysiology and Detailed Mechanism of Onset
Cytokine storm: SARS-CoV-2 activates inflammatory cells (neutrophils, monocytes) and endothelial cells, leading to elevated levels of inflammatory cytokines such as CRP, ferritin, IL-2, and TNF-α in the blood.
Hypercoagulability: Overproduction of tissue factor and von Willebrand factor leads to a procoagulant state.
Hypoxemia: Clinically significant hypoxemia due to COVID-19 is thought to cause thrombosis in capillaries and other vessels, leading to optic nerve ischemia.
Mechanism of ON
Autoimmune reaction: Molecular mimicry by SARS-CoV-2 induces autoantibodies against myelin proteins, causing demyelination.
MOG-IgG antibodies: MOG antibodies are produced, targeting oligodendrocytes, and demyelination occurs involving T cells and complement binding.
Neurotropism: SARS-CoV-2 can cross the blood-brain barrier and be transported to the central nervous system via infected leukocytes.
Onset patterns: There are parainfectious and postinfectious types, and the distinction remains unclear in some aspects.
Some reports have noted a decrease in the density of the peripapillary capillary network (radial peripapillary capillary network: RPCP) after COVID-19 infection, which is attracting attention as a finding suggesting the involvement of ischemia. It is known that even a negative RT-PCR in cerebrospinal fluid (CSF) cannot completely rule out central nervous system infection.
7. Latest Research and Future Perspectives (Research-stage Reports)
The pathogenesis of COVID-19-associated optic neuropathy has not yet been fully elucidated, and in particular, the ischemic origin of COVID-19 in ION has not been confirmed. Further research is needed.
Current areas of high research interest are listed below.
Association with vaccination: Cases of non-arteritic anterior ischemic optic neuropathy and ON after COVID-19 vaccination have been reported, and the combination of infection and vaccination may enhance immune responses. Elucidating the mechanism and determining the frequency are challenges.
Distinction between infection-associated and post-infectious ON: There are still no clear criteria for distinguishing between the two, and systematic research is needed.
Monitoring of long-term complications: Other neurological complications (e.g., Guillain-Barré syndrome, acute transverse myelitis) and future demyelinating diseases (e.g., multiple sclerosis) may develop after COVID-19, and long-term follow-up systems are considered important.
Biomarkers using OCT: Evaluation of peripapillary blood flow, including changes in RPCP density, is being studied as an early detection indicator of optic nerve ischemia.
Abdul-Salam (State) SE, Sfredel V, Mocanu CL, Albu CV, Bălășoiu AT. Optic neuropathies post-Covid 19 - review.Romanian Journal of Ophthalmology. 2022;66(4):289-298. PMID: 36589322. PMCID: PMC9773110. https://pmc.ncbi.nlm.nih.gov/articles/PMC9773110/
Jossy A, Jacob N, Sarkar S, Gokhale T, Kaliaperumal S, Deb AK. COVID-19-associated optic neuritis - A case series and review of literature.Indian Journal of Ophthalmology. 2022;70(1):310-316. PMID: 34937266. https://pubmed.ncbi.nlm.nih.gov/34937266/
Rho J, Dryden SC, McGuffey CD, Fowler BT, Fleming J. A Case of Non-Arteritic Anterior Ischemic Optic Neuropathy with COVID-19.Cureus. 2020;12(12):e11950. PMID: 33425529. PMCID: PMC7785499. https://pmc.ncbi.nlm.nih.gov/articles/PMC7785499/
Feizi M, Isen DR, Tavakoli M. Neuro-ophthalmic Manifestations of Coronavirus Disease 2019 and Its Vaccination: A Narrative Review.Journal of Ophthalmic & Vision Research. 2023;18(1):113-122. PMID: 36937195. https://pubmed.ncbi.nlm.nih.gov/36937195/
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.