Compressive visual field defects are a general term for visual field changes caused by compression of the visual pathway due to mass effect. Masses include tumors, aneurysms, hematomas, abscesses, and cysts.
The pattern of visual field defects varies greatly depending on which part of the visual pathway is compressed. Therefore, it is clinically very important to be able to estimate the location of the lesion from the pattern of visual field defects.
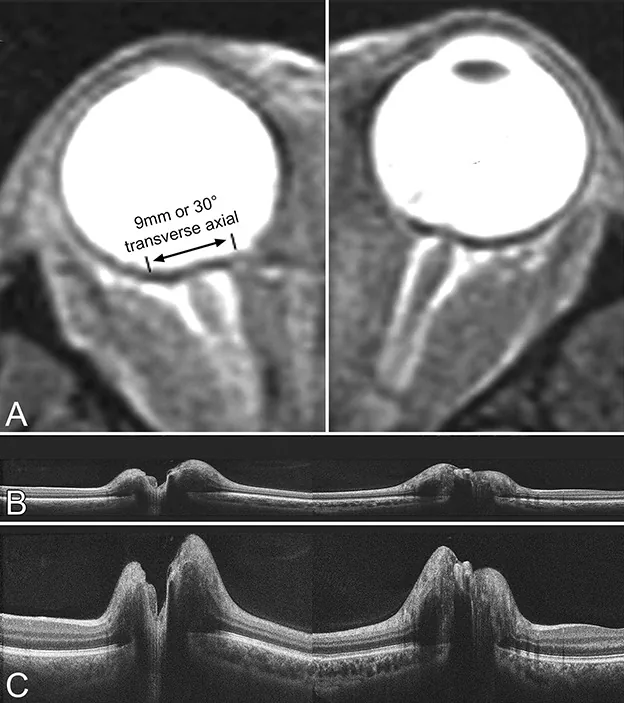
Sibony PA, et al. Optical Coherence Tomography Neuro-Toolbox for the Diagnosis and Management of Papilledema, Optic Disc Edema, and Pseudopapilledema. J Neuroophthalmol. 2021. Figure 1. PMCID: PMC7882012. License: CC BY.
A is an MRI image showing optic nerve sheath dilation and globe flattening, B and C are cross-sectional and vertically magnified OCT images, respectively. These correspond to the optic nerve compression findings discussed in the section “2. Main symptoms and clinical findings.”
Bitemporal hemianopsia: A classic finding caused by compression of crossing nasal fibers. Often asymmetric and incomplete.
Junctional scotoma: Central scotoma in the affected eye plus contralateral superior temporal visual field defect, suggesting an anterior chiasmal lesion.
Band optic atrophy: In the chronic phase, pallor of the temporal and nasal central optic disc.
Postchiasmal Lesions
Optic tract: Incongruous homonymous hemianopsia with RAPD. Near the cerebral peduncle, contralateral hemiparesis may occur.
Temporal lobe: Homonymous superior quadrantanopsia (“pie in the sky”). Reflects damage to Meyer’s loop.
Parietal lobe: Homonymous inferior quadrantanopia (“pie on the floor”). May be accompanied by Gerstmann syndrome and hemispatial neglect.
In compressive optic neuropathy, the optic disc initially swells and progresses to pallor and atrophy if treatment is delayed. Optical coherence tomography (OCT) detects localized thinning of the inner retinal layers corresponding to visual field defects.
In compressive optic neuropathy due to sphenoid fibrous dysplasia, glaucomatous-like cupping has been reported, with OCT showing thinning of the retinal nerve fiber layer (RNFL) in all quadrants and diffuse loss of the ganglion cell layer5).
QWhat visual field defect patterns other than bitemporal hemianopia can occur?
A
At the anterior chiasm, junctional scotoma (central scotoma in the affected eye plus contralateral superior temporal defect) or Traquair junctional scotoma (monocular hemianopic defect) may occur. Posterior to the chiasm, homonymous hemianopia or quadrantanopia appears depending on the compression site.
Extraconal: Lymphoma (most common malignant), metastatic tumors (breast and lung cancer common in adults), lacrimal gland tumors, invasion of paranasal sinus tumors, etc.
Intercompartmental: Lymphangioma, neurofibroma (plexiform/diffuse), capillary hemangioma, etc.
Humphrey automated perimetry (24-2, 30-2, 10-2) is recommended for all patients with unexplained visual impairment. The pattern of visual field defects helps estimate the compression site and determine the imaging strategy.
Visual field testing is also useful for assessing disease progression and treatment efficacy, and should be performed over time.
Excellent for detecting bone lesions, calcifications, and bone destruction
Orbital bone lesions, surgical planning
MRI
Best for soft tissue evaluation. Gold standard.
Tumor characterization, optic nerve assessment
PET/CT
Search for systemic metastases
Staging of malignant tumors
On T2-weighted MRI, it is useful for differentiating tumor characteristics. Solid tumors (such as lymphoma and meningioma) appear hypo- to isointense, while vascular and cystic tumors (such as cavernous hemangioma and dermoid cyst) appear hyperintense. Dynamic MRI is also useful in contrast-enhanced MRI, and delayed enhancement is characteristic of cavernous hemangioma.
Optical coherence tomography (OCT) detects localized thinning of the inner retinal layers and is useful for early detection of mild optic atrophy. It can detect abnormalities earlier than visual field testing. It also helps in estimating prognosis after treatment.
Compressive optic neuropathy may present with glaucomatous cupping of the optic disc5). The following findings suggest a non-glaucomatous etiology.
Age under 50 years
Headache or periorbital pain
Visual field defect affecting the vertical meridian
Rapid visual acuity decline
Pallor disproportionate to optic disc cupping
Asymmetric visual acuity loss and visual field defect
A report indicates that 6.5% of patients diagnosed with normal-tension glaucoma had clinically significant intracranial compressive lesions5).
QHow is glaucoma distinguished from compressive optic neuropathy?
A
Glaucoma presents with arcuate scotomas along the horizontal nerve fiber bundle, whereas compressive optic neuropathy is characterized by visual field defects that respect the vertical meridian. Pallor disproportionate to cupping, rapid vision loss, and onset before age 50 suggest a compressive lesion. If suspected, neuroimaging should be performed.
Most mass lesions compressing the visual pathway require surgery for both diagnosis (pathological confirmation) and treatment (relief of mass effect). Multidisciplinary collaboration (ophthalmology, neurosurgery, otolaryngology, endocrinology, etc.) depending on the cause is essential.
Pituitary adenoma: Surgery is the first choice except for prolactinomas. For prolactinomas, drug therapy such as bromocriptine or cabergoline is the mainstay. For other brain tumors, radiation therapy is also performed in addition to surgery.
Orbital tumor: Complete surgical resection is the standard for benign tumors. Pleomorphic adenoma of the lacrimal gland has a high recurrence rate with simple enucleation.
Malignant lymphoma: Highly radiosensitive. For localized orbital lymphoma, approximately 30 Gy is administered; for moderate to high grade, approximately 40 Gy.
Metastatic tumor: Hormone therapy may be effective for breast and prostate cancer. Systemic chemotherapy is also used in combination.
Thyroid eye disease: Steroid pulse or half-pulse therapy is first-line. After 1–3 courses, switch to oral administration. Orbital decompression is performed for steroid-resistant cases. With appropriate treatment, approximately 70% or more recover visual function.
Paranasal sinus mucocele: Emergency endoscopic sinus surgery for decompression is first-line1)4). Initial visual acuity is considered an important prognostic factor1).
Fibrous dysplasia: Surgical decompression is considered for symptomatic optic nerve compression. The indication for surgery in asymptomatic cases is debated5).
Once the compression of the optic chiasm is relieved, improvement in visual acuity and visual field can be observed. However, if optic atrophy is already evident, the visual prognosis is poor. Measurement of retinal thickness using OCT is useful for estimating prognosis after treatment.
In compressive optic neuropathy, a delay in intervention of 7 to 10 days or more is associated with an increased risk of irreversible visual impairment4).
QWill vision recover if optic nerve compression is relieved?
A
Relief of compression can improve visual acuity and visual field. However, recovery is limited if optic atrophy has progressed. Better initial visual acuity indicates a better prognosis.
At the optic chiasm, nasal retinal fibers cross to the opposite side, while temporal retinal fibers remain uncrossed and proceed ipsilaterally. Nasal fibers process the temporal visual field, and temporal fibers process the nasal visual field. Therefore, compression of crossing fibers causes temporal visual field defects, while compression of non-crossing fibers causes nasal visual field defects.
The Wilbrand knee (a structure where contralateral inferior nasal retinal fibers briefly enter the ipsilateral optic nerve before crossing) has been proposed as a cause of junctional scotoma, but its existence is debated.
The optic radiation emerges dorsally from the LGN and divides into two bundles.
Inferior fiber group (Meyer loop): Loops around the temporal lobe and transmits information from the upper visual field. Temporal lobe lesions cause homonymous superior quadrantanopia.
Superior fiber group (parietal bundle): Passes through the deep parietal lobe and transmits information from the lower visual field. Parietal lobe lesions cause homonymous inferior quadrantanopia.
The tip of the occipital cortex (macular representation area) receives dual blood supply from the middle cerebral artery and posterior cerebral artery, so macular sparing can occur with damage to a single vascular territory.
Direct compression: Physical compression of the optic canal by a mass causes axonal damage.
Blood flow impairment: Compression disrupts blood supply to the optic nerve.
Inflammatory spread: The infected contents of the mucocele spread directly to the optic nerve sheath.
The effect of the tumor on the optic chiasm involves both direct compression and inflammatory blood flow disturbance.
In temporal lobe lesions caused by compressive lesions, the visual field defect shows a gradual isopter pattern compared to vascular lesions.
Blood flow to the LGN is supplied by the anterior choroidal artery and posterior choroidal artery. Segmental homonymous visual field defects occur depending on the site of damage to each small artery.
7. Latest Research and Future Perspectives (Research Stage Reports)
Teprotumumab (IGF-1R inhibitory monoclonal antibody) is the first approved drug for thyroid eye disease. Patients with compressive optic neuropathy (CON) were excluded from clinical trials, but efficacy has been reported in mild CON cases.
Chiou et al. (2021) reported two cases of mild CON due to thyroid eye disease that were resistant to IV steroids; after treatment with teprotumumab, visual field defects completely resolved in both cases 3). In the first case, resolution was observed after the third dose, and in the second case after the second dose.
Management of Aneurysm Enlargement After Flow Diverter Placement
Tsuei et al. (2022) reported a case of a 17 mm paraclinoid internal carotid artery aneurysm treated with a flow diverter (Pipeline embolization device). Despite complete angiographic occlusion, the aneurysm enlarged and caused compressive optic neuropathy8). Visual fields improved after microsurgical optic nerve decompression and coagulation shrinkage of the aneurysm.
Zhou et al. (2024) performed endoscopic endonasal optic nerve decompression (ETOND) in four adolescent patients (mean age 12.75 years, all male) with visual impairment due to pneumosinus dilatans of the sphenoid bone 10). All cases were resistant to steroid pulse therapy, but visual improvement was achieved with ETOND.
Treatment Limitations of Compressive Optic Neuropathy Due to Malignant Tumors
Kong et al. (2022) reported a case of bilateral orbital apex infiltration due to nasopharyngeal carcinoma leading to loss of light perception 7). Despite treatment with steroids, chemotherapy, and radiotherapy, the right eye had no light perception and the left eye only hand motion. The optic nerve is considered to have the lowest recovery rate among cranial nerves 7).
Haydar et al. (2024) reported a case of compressive optic neuropathy caused by a hydatid cyst within the inferior rectus muscle in a 22-year-old male from Afghanistan 9). Complete excision and long-term albendazole therapy restored vision from 20/200 to 20/20.
Che SA, Lee YW, Yoo YJ. Compressive optic neuropathy due to posterior ethmoid mucocele. BMC ophthalmology. 2023;23(1):426. doi:10.1186/s12886-023-03168-w. PMID:37867195; PMCID:PMC10591398.
Teng Siew T, Mohamad SA, Sudarno R, et al. Unilateral proptosis and bilateral compressive optic neuropathy in a meningioma patient. Cureus. 2024;16(2):e53728.
Chiou CA, Reshef ER, Freitag SK. Teprotumumab for the treatment of mild compressive optic neuropathy in thyroid eye disease: A report of two cases. American journal of ophthalmology case reports. 2021;22:101075. doi:10.1016/j.ajoc.2021.101075. PMID:33889787; PMCID:PMC8050009.
Deb AK, Neena A, Sarkar S, et al. Bilateral compressive optic neuropathy secondary to sphenoid sinus mucocele mimicking bilateral retrobulbar neuritis. Saudi J Ophthalmol. 2021;35:368-370. doi:10.4103/1319-4534.347312.
Kiyat P, Top Karti D, Esen Ö, Karti Ö. Sphenoid bone dysplasia: a rare cause of compressive optic neuropathy mimicking glaucoma. Turk J Ophthalmol. 2023;53:70-73.
Hassan MN, Wan Hitam WH, Masnon NA, Govindasamy S, Omar AR. Compressive Optic Neuropathy Secondary to Sinonasal Undifferentiated Carcinoma in a Young Male. Cureus. 2021;13(10):e19042. doi:10.7759/cureus.19042. PMID:34858739; PMCID:PMC8612748.
Kong Y, Ng GJ. Rare early presentation of bilateral compressive optic neuropathy with complete vision loss from nasopharyngeal carcinoma. BMJ case reports. 2022;15(3). doi:10.1136/bcr-2022-248902. PMID:35232748; PMCID:PMC8889247.
Tsuei YS, Fu YY, Chen WH, Cheng WY, Liao CH, Shen CC. Compressive optic neuropathy caused by a flow-diverter-occluded-but-still-growing supraclinoid internal carotid aneurysm: illustrative case. Journal of neurosurgery. Case lessons. 2022;4(1):CASE22139. doi:10.3171/CASE22139. PMID:35855353; PMCID:PMC9257398.
Haydar AA, Rafizadeh SM, Rahmanikhah E, Nozarian Z, Aghajani A, Rajabi MT. Orbital intramuscular hydatid cyst causing compressive optic neuropathy: a case report and literature review. BMC ophthalmology. 2024;24(1):257. doi:10.1186/s12886-024-03502-w. PMID:38877497; PMCID:PMC11179359.
Zhou X, Xu Q, Zhang B, Liu Y, Liu X, Wang S, et al. Sphenoidal pneumosinus dilatans associated compressive optic neuropathy: A case series of four adolescent patients. Heliyon. 2024;10(20):e38763. doi:10.1016/j.heliyon.2024.e38763. PMID:39640786; PMCID:PMC11620074.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.