Glioblastoma multiforme (GBM) is an astrocytoma classified as WHO grade 4 and is the most common primary malignant brain tumor in adults. The incidence in the United States is approximately 3 per 100,000 people, with more than 10,000 cases diagnosed annually. It accounts for 12–15% of all brain tumors and 45.2% of malignant CNS tumors 3). The mean age at diagnosis is 64 years, and the male-to-female ratio is 1.5:1.
Neuro-ophthalmic signs arise from one or a combination of the following three mechanisms.
Direct occurrence/infiltration: Direct occurrence or infiltration of the tumor into the optic nerve, optic chiasm, or optic tract
Compression: Compression of the visual pathway due to mass effect from surrounding structures
Increased intracranial pressure: Papilledema associated with elevated brain pressure caused by the tumor
Primary optic nerve GBM is extremely rare, accounting for 0.6–1.2% of all brain tumors, with only about 70 cases reported in the literature1). Adult-type optic glioma is highly malignant and commonly occurs in middle-aged men. The prognosis is approximately 6 months, following a completely different course from the pediatric type.
The mean survival time when the visual pathway is involved is about 8 months, shorter than the 14.6 months for non-visual pathway GBM.
QHow rare is glioblastoma occurrence in the optic pathway?
A
Primary optic nerve glioblastoma accounts for 0.6–1.2% of all brain tumors, with only about 70 cases reported worldwide 1). It is a very rare condition, and attention is needed as diagnosis is often delayed.
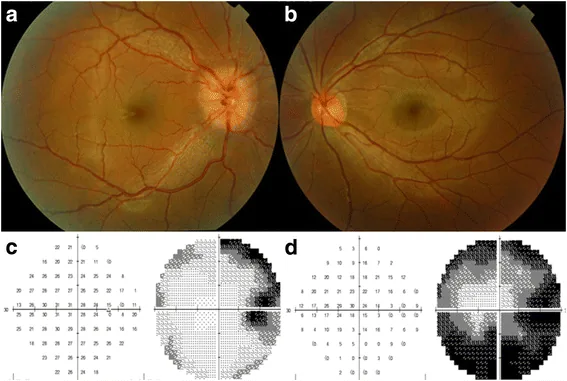
Chia-Ying Lin, Hsiu-Mei Huang. Unilateral malignant optic glioma following glioblastoma multiforme in the young: a case report and literature review. BMC Ophthalmology. 2017 Mar 11; 17:21. Figure 1. PMCID: PMC5346192. License: CC BY.
Decreased visual acuity: Unilateral or bilateral. Occurs due to involvement of the optic nerve or optic chiasm. In adult-type optic glioma, it may present with unilateral vision loss and progress to bilateral blindness within weeks as it infiltrates the optic chiasm.
Visual field defects: Follow a pattern corresponding to the tumor location (see below).
Proptosis: Occurs when the tumor arises from the optic nerve. In the case reported by Brokāns, the patient presented with left proptosis, decreased vision, and limited upward gaze for 6 months1).
Headache: Due to increased intracranial pressure or direct tumor effect.
Bitemporal hemianopia: Involvement of the optic chiasm. May be accompanied by junctional scotoma.
Contralateral homonymous hemianopia: Involvement of the retrochiasmal region (optic tract and optic radiation).
Band atrophy of the optic nerve: Appears with contralateral RAPD when the optic tract is involved. Characterized by pallor of the temporal and nasal optic disc margins.
Tectal RAPD: In midbrain tectal lesions, RAPD may occur without visual impairment.
Papilledema due to increased intracranial pressure initially presents only with blurred vision and enlargement of the Mariotte blind spot. If it persists for a long time, optic atrophy occurs, and visual field narrowing and visual acuity loss progress.
The direction of MRI imaging varies depending on the lesion site. For lesions anterior to the optic chiasm, coronal orbital sections are essential; for posterior lesions, axial brain sections are useful.
QWhat pattern of visual field defect occurs in glioblastoma?
A
The pattern of visual field defect varies depending on the tumor location. Involvement of the optic nerve causes ipsilateral central scotoma and peripheral visual field loss; involvement of the optic chiasm causes bitemporal hemianopia; involvement posterior to the chiasm (optic tract or optic radiation) causes contralateral homonymous hemianopia.
Approximately 95% of GBM cases are sporadic, and only about 5% are associated with hereditary syndromes. Occurrence is broadly divided into primary and secondary types, which have different molecular profiles.
The main molecular changes in primary and secondary types are shown below.
Factors associated with the risk of extracranial metastasis include TP53, TERT, and PTEN mutations, chromosome +7/−10, and sarcomatoid histology6). Risk factors for leptomeningeal dissemination include ventricular opening, repeat surgery, male sex, and ependymal invasion3).
MRI (first choice): The combination of T1 contrast enhancement and T2/FLAIR hyperintensity is characteristic. For lesions anterior to the optic chiasm, add coronal orbital sections 1).
CT: Used for screening and detection of bone or calcification 1).
OCT: Detects thinning of the retinal nerve fiber layer and ganglion cell layer. It has high sensitivity for detecting subtle optic atrophy and is useful for identifying early lesions.
Visual Field Testing: Evaluates visual field defect patterns corresponding to the tumor location. It helps estimate the lesion site, such as bitemporal hemianopia or homonymous hemianopia.
RAPD assessment: Strongly suggests optic nerve pathology; a simple and important finding.
The goal is resection to the maximum safe extent. In primary optic nerve GBM, complete resection is often difficult due to proximity to visual structures 1). In Japan, observation, surgery, chemotherapy, and radiotherapy are selected based on tumor location and progression.
Decompression of the optic chiasm may improve visual acuity. However, in cases with advanced optic atrophy, visual recovery is unlikely even after decompression, leading to a poor prognosis.
Leptomeningeal seeding occurs in 2–4% (up to 15–25%) of GBM cases, with survival ranging from 0.2 to 9.7 months2). Primary LMS is extremely rare. No standard treatment exists; intrathecal chemotherapy and additional radiation have limited efficacy.
QCan optic nerve glioblastoma be completely resected?
A
Because primary optic nerve GBM is adjacent to visual structures, complete resection is often difficult when prioritizing functional preservation 1). It is common to perform maximal safe resection followed by radiation and chemotherapy.
The central pathway of GBM proliferation, invasion, and angiogenesis is activation of the RAS/PI3K pathway via EGFR amplification. Additionally, immunosuppression in the tumor microenvironment is characteristic, with lack of T cell infiltration and increases in regulatory T cells (Treg) and myeloid-derived suppressor cells (MDSC) promoting immune evasion 4).
The main route of dissemination is via the subarachnoid space 3). Autopsy reveals spinal dissemination in 25% of cases.
Effects on the optic pathway arise from the following three mechanisms.
Direct occurrence/infiltration: Direct occurrence or infiltrative spread of tumor into the optic nerve, optic chiasm, optic tract, or optic radiation
Compression: Compression and deformation of the visual pathway by an adjacent tumor mass
LITT induces coagulative necrosis at temperatures above 46°C, while at 33–43°C it opens the BBB (blood-brain barrier) and induces immunogenic cell death4).
Chandar et al. (2023) performed LITT in a case of newly diagnosed GBM and confirmed a marked increase in CD8+ T cells and PD-L1 after treatment 4). The patient achieved 9-year recurrence-free survival.
Long et al. (2025) administered a triple-drug ICI regimen of nivolumab, ipilimumab, and relatlimab before surgery in newly diagnosed GBM 5). After treatment, tumor-infiltrating CD3+ T cells increased from 9.8% to 32.7%, and activated T cells increased 8.5-fold. One case showed recurrence-free survival for 17 months, and the GIANT trial is currently planned.
QIs immunotherapy effective for glioblastoma?
A
Immunotherapy as a standard treatment has not been established at this time. However, neoadjuvant triple-agent ICI administration has been shown to markedly increase intratumoral T-cell infiltration5), and further validation in clinical trials is expected.
Extracranial metastasis occurs in 0.4–2.0% of GBM cases, and the median survival after metastasis is extremely short at 1.5 months6). TP53, TERT, and PTEN mutations have been reported as molecular features of metastatic cases, and these are being studied as biomarkers for metastasis risk6).
Brokāns A, Dolgopolova J, Saulītis A, et al. Optic Nerve Glioblastoma with Optic Chiasm Involvement: A Case Report and a Brief Literature Review. Medicina. 2024;60(10):1687. doi:10.3390/medicina60101687.
Mondia MWL, Hooks RE, Maragkos GA, Smith VL, McCord MR, Donahue JH, et al. Primary diffuse leptomeningeal glioblastoma: a case report and literature review. Journal of neuro-oncology. 2025;172(1):265-272. doi:10.1007/s11060-024-04908-8. PMID:39666263; PMCID:PMC11832630.
Zhang K, Yang Y, Zhuang J, Guo G, Chao X, Zhang Z. Intracranial dissemination of glioblastoma multiforme: a case report and literature review. The Journal of international medical research. 2022;50(7):3000605221112047. doi:10.1177/03000605221112047. PMID:35854630; PMCID:PMC9310070.
Chandar JS, Bhatia S, Ingle S, Mendez Valdez MJ, Maric D, Seetharam D, et al. Laser Interstitial Thermal Therapy Induces Robust Local Immune Response for Newly Diagnosed Glioblastoma With Long-term Survival and Disease Control. Journal of immunotherapy (Hagerstown, Md. : 1997). 2023;46(9):351-354. doi:10.1097/CJI.0000000000000485. PMID:37727953; PMCID:PMC10591996.
Long GV, Shklovskaya E, Satgunaseelan L, Mao Y, da Silva IP, Perry KA, et al. Neoadjuvant triplet immune checkpoint blockade in newly diagnosed glioblastoma. Nature medicine. 2025;31(5):1557-1566. doi:10.1038/s41591-025-03512-1. PMID:40016450; PMCID:PMC12092302.
Yuen CA, Pekmezci M, Bao S, Kong XT. Metastatic glioblastoma to the lungs: a case report and literature review. CNS Oncol. 2024;13(1):2351789. doi:10.1080/20450907.2024.2351789.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.