Painful blind eye (PBE) is defined as an eye with visual acuity of counting fingers or less, no potential for functional recovery, and chronic pain or discomfort lasting more than 4 weeks 1).
It is estimated that 1 in 10 blind individuals have PBE 1)2). The most common cause is various types of glaucoma including neovascular glaucoma; trauma, corneal degeneration, chronic inflammation, retinal detachment, and sequelae of endophthalmitis are also causes 1). In many cases, symptoms are refractory to initial treatment and significantly reduce the patient’s quality of life 1).
Currently, there are no unified guidelines for PBE management, and most treatments are based on experience 1).
QHow common is painful blind eye?
A
Approximately 1 in 10 blind individuals are estimated to have PBE 1)2). The most common cause is glaucoma; trauma, bullous keratopathy, and chronic uveitis are also causes of PBE.
Other causes include trauma, chronic retinal detachment, and failed corneal graft 1). In developing regions such as Africa, chemical trauma from traditional medicine (TEM) and limited access to healthcare are important factors for PBE 2).
Acute glaucoma attack causes severe eye pain, headache, and corneal edema due to rapid intraocular pressure elevation 3), and if not managed appropriately, can lead to PBE.
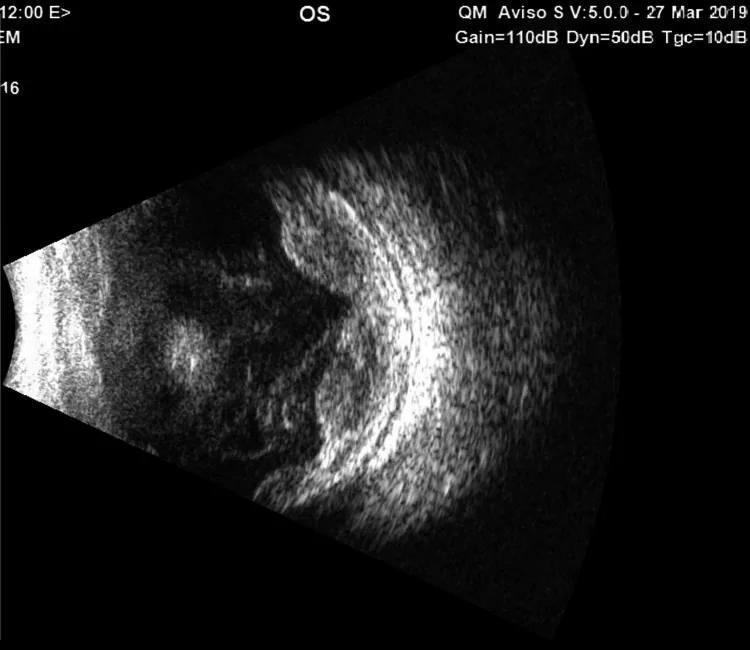
Hassanin FF, Elkhamary S, Al Thaqib R, et al. A Case of Escherichia coli Endogenous Panophthalmitis and Orbital Cellulitis With Normal Workup for Primary Focus. Cureus. 2021;13(5):e15103. Figure 2. PMID: 34159011; PMCID: PMC8212906; DOI: 10.7759/cureus.15103. License: CC BY.
B-scan ultrasound image showing choroidal detachment, vitreous strands, and scleral thickening. It is used as a diagnostic aid to detect posterior segment complications in a blind painful eye where the anterior segment is difficult to visualize.
For the diagnosis of PBE, it is important to first identify the cause of blindness and understand the mechanism of pain.
History taking: Obtain a detailed history of the cause and course of blindness, as well as the nature, duration, and aggravating factors of pain.
Visual acuity testing: Confirm no light perception (NLP). Evaluation of the contralateral eye is also essential.
Intraocular pressure measurement: Treatment strategy differs depending on whether intraocular pressure is high or low. Marked elevation is observed during acute attacks 3).
Slit-lamp examination: Evaluate corneal edema, epithelial bullae, band keratopathy, anterior synechiae, and rubeosis.
B-scan ultrasonography: Evaluate intraocular pathology (e.g., tumor, retinal detachment) when the fundus is not visible. Exclusion of intraocular malignancy is particularly important before enucleation1).
Examination of the contralateral eye: Assessment and follow-up of the healthy eye are essential.
Treatment of PBE is based on a stepwise approach 1). Conservative treatment is the first choice; if ineffective, minimally invasive treatment and ultimately enucleation are considered.
Conservative Treatment
Topical steroids: Mainly for inflammation control. Prednisolone eye drops 1–4 times daily 1).
Mydriatics: Atropine 1% twice daily. Stabilizes the blood-aqueous barrier and relieves ciliary spasm 1).
Intraocular pressure-lowering agents: Up to two classes of aqueous suppressants. The goal is symptom relief, not strict IOP control 1).
Artificial tears and ointments: For relief of ocular surface symptoms. Preservative-free formulations are preferred 1).
Therapeutic contact lenses: Effective for pain reduction in bullous keratopathy.
Minimally Invasive Treatment
Cyclophotocoagulation (CPC): Selected when high intraocular pressure is the main cause of pain. Transscleral diode laser CPC is the mainstream approach1).
Retrobulbar injection: Alcohol or chlorpromazine is injected behind the globe to block the ciliary nerves1).
Intravitreal triamcinolone: Effective when the inflammatory component is strong. Onset of effect from the first day has been reported1).
Gundersen conjunctival flap: Aims to protect the corneal surface and reduce pain1).
Transscleral diode laser CPC has been reported to reduce pain in PBE, with an intraocular pressure reduction of 30% or more being the best predictor of success (P = 0.0042)1).
Cyclocryotherapy is also effective, but the risk of hypotony and phthisis bulbi is higher than with CPC1). Ultrasound cycloplasty (UCP) is a newer technique that allows selective coagulation and is expected to reduce tissue damage1).
Selected for patients who do not respond to topical therapy and do not wish to undergo enucleation.
A comparison of retrobulbar alcohol injection and chlorpromazine injection showed that at 36 weeks, the efficacy rate was 43.7% (7/16) for alcohol and 37.5% (6/16) for chlorpromazine, with no significant difference (P = 0.6). Side effects included transient orbital irritation with chlorpromazine and more frequent extraocular muscle paresis with alcohol1).
PBE is thought to involve a component of neuropathic pain due to corneal nerve damage1). Gabapentin is a first-line drug for neuropathic pain, and its application to PBE has been reported.
A case has been reported in which gabapentin (up to 2,400 mg/day) was administered to a patient with glaucomatous PBE whose pain was poorly controlled even after cyclodestructive procedures. Pain relief was obtained from the first day of administration and persisted for 6 months1).
Anterior corneal stromal puncture: In a study of 14 cases of bullous keratopathy, significant pain improvement was shown from 1 to 24 weeks postoperatively (P < 0.0001)1)
This is a last resort when conservative or minimally invasive treatments fail, or when the eye is severely deformed or disintegrated1).
There are reports that enucleation and evisceration have equivalent pain relief effects. Observational studies have shown that prosthetic eye motility is better with evisceration (70% of normal vs 54%), but there were no significant differences in cosmetic outcomes or complications1).
Before removal surgery, it is important to rule out intraocular malignancy by ultrasound1). The risk of sympathetic ophthalmia is rare (0.01–0.3%), but it increases with a history of penetrating trauma or multiple intraocular surgeries1).
QWhat are the drugs used in retrobulbar injection and their differences in effect?
A
Mainly alcohol (100%) and chlorpromazine are used. A randomized controlled trial showed no significant difference in efficacy at 36 weeks1). Side effects: chlorpromazine tends to cause transient orbital irritation, while alcohol more often causes extraocular muscle paresis.
QWhich should I choose: enucleation or evisceration?
A
Both procedures are reported to have equivalent pain relief effects1). Evisceration is said to provide better prosthetic eye motility, but there are no clear differences in cosmetic outcomes or complications. Enucleation is recommended if there is a possibility of intraocular tumor. The choice depends on patient preference, general condition, and structural integrity of the eye.
Sustained elevation of intraocular pressure causes corneal endothelial damage. When the endothelial pump function falls below a threshold (generally ≤500 cells/mm²), corneal edema becomes irreversible. Bullae form under the epithelium, and their rupture leads to recurrent severe pain. Further progression results in vascular invasion from the corneal periphery and stromal scarring with opacification.
Chronic uveitis or ocular ischemia leads to sustained release of inflammatory mediators, inducing ciliary spasm and causing pain 1). The efficacy of steroid eye drops and mydriatics is based on this mechanism.
In PBE, peripheral nerve sensitization via corneal nerve damage and maladaptive central neuroplasticity are thought to be involved 1). This mechanism provides the rationale for the effectiveness of gabapentinoids.
During the progression of chronic inflammation or phthisis bulbi, calcium deposits in the corneal stroma can cause band keratopathy. This itself can cause foreign body sensation and pain. Treatment includes chelation with EDTA or dissolution with dilute hydrochloric acid.
Ultimately, when ciliary body function fails and aqueous humor production ceases, the eye becomes atrophic and deformed (phthisis bulbi) 2). Pain may persist at this stage, and enucleation may be indicated.
There is no unified guideline for PBE management. Parra-Tanoux et al. (2023) proposed a stepwise management algorithm based on available evidence, but noted that evidence is lacking for many treatments and pointed out the need for large-scale studies 1).
Ultrasound cycloplasty (UCP) is a technique that minimizes tissue damage through selective coagulation and micropulse irradiation 1), and is expected to be applied to PBE. Comparative clinical trials with conventional transscleral CPC are needed in the future.
Stellate ganglion block (once a week for 6 sessions) has been reported to maintain pain-free status or allow pain control with adjunctive medication in more than half of patients with glaucomatous PBE at one-year follow-up 1).
This technique requires collaboration with a multidisciplinary pain management team, and accumulation of evidence is awaited.
In Africa, the prevalence of PBE is high, but the number of ophthalmologists is severely insufficient 2). The dissemination of minimally invasive treatments such as CPC and retrobulbar injection, as well as the establishment of initial response systems at the primary care level, are cited as challenges 2).
Parra-Tanoux D, Dussan-Vargas MP, Gonzalez Escandon M. Painful-blind eye: A forgotten palliative care. Indian J Ophthalmol. 2023;71(6):2399-2408.
Kayoma DH, Oronsaye DA. Management of painful blind eye in Africa: A review. Journal of the West African College of Surgeons. 2024;14(3):245-248. doi:10.4103/jwas.jwas_164_23. PMID:38988421; PMCID:PMC11232782.
日本緑内障学会. 緑内障診療ガイドライン(第5版). 日本眼科学会雑誌. 2022.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.