Immune checkpoint inhibitors (ICIs) are monoclonal antibodies that block checkpoint molecules, which act as brakes on T cells, thereby enhancing the immune response against cancer cells 1). While they have revolutionized cancer treatment, they also cause immune-related adverse events (irAEs) — non-specific inflammation in tissues other than tumors 1).
The main target molecules and representative drugs are listed below 1).
Target molecule
Representative drugs
CTLA-4
Ipilimumab, Tremelimumab
PD-1
Pembrolizumab, Nivolumab, Cemiplimab
PD-L1
Atezolizumab, Avelumab, Durvalumab
CTLA-4 suppresses T cell activation through interaction with costimulatory molecules CD80/CD86 on T cell surfaces 1). PD-1 is a receptor on activated T cells that inhibits immune responses when bound to PD-L1 on antigen-presenting cells or tumor cells 1). Inhibition of these pathways promotes T cell activation and antitumor immunity, but can also trigger autoimmune reactions.
The incidence of ocular irAE is 1–3%, mainly presenting as ocular surface disease (dry eye) and anterior uveitis1). Inflammation of the posterior segment (retina/choroid) accounts for approximately 5–20% of all ocular irAE, but is more severe and can lead to permanent vision loss if not properly managed 1).
QHow often do ocular side effects of immune checkpoint inhibitors occur?
A
Ocular immune-related adverse events (irAE) occur at a frequency of 1–3% 1). Most are dry eye or anterior uveitis, but posterior segment inflammation (5–20%) can be a serious complication affecting visual prognosis.
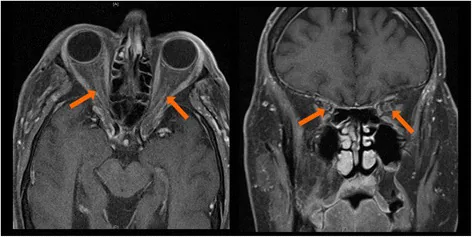
Melissa A Wilson, Kelly Guld, Steven Galetta, Ryan D Walsh, et al. Acute visual loss after ipilimumab treatment for metastatic melanoma 2016 Oct 18 J Immunother Cancer. 2016 Oct 18; 4:66 Figure 3. PMCID: PMC5067900. License: CC BY.
Axial and coronal MRI show ring-shaped contrast enhancement around both optic nerves. This is an inflammatory finding in the posterior orbit indicating optic neuritis.
Symptoms vary depending on the site and severity. Dry eye mainly causes dryness and foreign body sensation. Uveitis causes redness, blurred vision, and photophobia. Orbital myositis presents with diplopia, ptosis, and proptosis2). Posterior segment inflammation leads to vision loss and floaters1).
Retinal vasculitis: Accompanied by vascular leakage and macular edema. Both arterial and venous occlusions have been reported 1).
Choroidal granuloma: Reported with nivolumab as a sarcoid-like reaction 1).
Orbit
Orbital myositis: Often bilateral. MRI shows enlargement and contrast enhancement of extraocular muscles2).
Orbital fat inflammation: May extend to the orbital apex and superior orbital fissure2).
Thyroid eye disease-like inflammation: Can occur even in patients with normal thyroid function.
Neurologic
Ocular myasthenia gravis: Associated with anti-AChR antibody production. Reported with pembrolizumab.
Optic neuritis: Early steroid treatment can preserve vision.
Abducens nerve palsy: Improves with drug discontinuation plus high-dose steroids.
The onset of orbital inflammation ranges from 2 days to 2 months after the first dose2). It may be accompanied by systemic symptoms (fatigue, fever, gastrointestinal symptoms, systemic myositis, myocarditis)2).
The root cause of ocular irAEs from ICIs is the induction of autoimmune reactions due to the release of T-cell immune checkpoints1).
CTLA-4 inhibition: Releases the brake that controls T-cell activation, allowing attacks not only on cancer cells but also on normal tissues1)
PD-1/PD-L1 inhibition: Enhances T-cell responses in the tumor microenvironment but simultaneously disrupts PD-L1-dependent immune privilege in ocular tissues1)
Vulnerability of ocular immune privilege: In normal eyes, the blood-retinal barrier (BRB) and lack of lymphatics prevent T-cell infiltration, but conditions with pre-existing BRB disruption, such as diabetic retinopathy, increase the risk1)
Host genetic predisposition: Genetic background contributes to the development of autoinflammatory events1)
Combination therapy: Combining anti-CTLA-4 and anti-PD-1/PD-L1 increases the risk of irAEs
QWhy do immune checkpoint inhibitors cause eye inflammation?
A
ICIs release T-cell immune checkpoints to attack cancer, but they also simultaneously disrupt the PD-L1-dependent immune privilege of ocular tissues 1). For details, three main mechanisms are explained in the “Pathophysiology” section.
The diagnosis of ICI-related ocular irAE is based on the temporal relationship between ICI use and ocular findings. The following examinations are used.
Slit-lamp microscopy: Evaluation of anterior chamber inflammatory cells, flare, and corneal findings
Fundus examination: Detection of retinal vasculitis, subretinal fluid, and choroidal granulomas
Optical coherence tomography (OCT): Evaluation of loss of outer retinal layers, hyperreflective retinal dots, subretinal fluid, and choroidal thickening 1)
Fluorescein angiography (FA): Evaluation of vascular leakage, macular edema, and vascular occlusion 1)
Electroretinography (ERG): Detection of rod and cone dysfunction in MAR-like retinopathy
MRI: Detection of extraocular muscle enlargement, contrast enhancement, and inflammatory changes in orbital fat in orbital myositis 2)
ICI-related ocular irAEs mimic various known eye diseases. Anterior uveitis requires differentiation from infectious and non-infectious uveitis. VKH-like reactions are clinically similar to primary VKH, but a history of ICI use for melanoma is an important clue 1). Orbital myositis requires differentiation from thyroid eye disease, IgG4-related disease, and idiopathic orbital inflammation2).
ICI discontinuation: Rarely necessary; in most cases, it can be managed with steroid therapy while continuing ICI
QIf ocular side effects of immune checkpoint inhibitors occur, should the drug be discontinued?
A
Discontinuation of ICI is rarely necessary. Most ocular irAEs can be controlled with steroids (eye drops, local injection, systemic administration), and it is common to continue ICI treatment while managing ophthalmologically. However, in severe cases, discontinuation should be considered in consultation with the oncologist.
Haliyur et al. (2025) proposed classifying ICI-induced posterior segment irAEs into the following three types 1).
Type 1
T cell cross-reactivity and autoreactivity expansion
Type 1a: Antitumor T cells cross-react with ocular tissues such as melanin-containing cells, triggering VKH-like panuveitis1). This accounts for 5–14% of VKH-like reactions in melanoma patients.
Type 1b: Pre-existing ocular tissue-resident memory T cells are expanded and activated by ICIs 1), leading to autoimmune retinopathy.
Type 2
Bystander effect-induced vasculitis
Systemic inflammation enhanced by ICI use nonspecifically disrupts the blood-retinal barrier1).
Perivascular lymphoplasmacytic infiltration by CD4-positive T cells and upregulation of adhesion molecules cause retinal vasculitis and arteriovenous occlusion 1).
Type 3
Autoantibody-mediated inflammation
PD-1 is also expressed on B cells, and ICIs induce expansion of B cell lineages and production of tissue-specific autoantibodies from plasma cells 1).
It is also involved in exacerbation of paraneoplastic syndromes (such as MAR-like retinopathy) 1).
Haliyur et al. (2025) proposed a three-mechanism classification for ICI-induced posterior segment irAE 1). Type 1 involves T-cell cross-reactivity with ocular tissues (1a) and expansion of autoreactive T cells (1b), Type 2 involves retinal vasculitis due to bystander effects, and Type 3 involves autoantibody-mediated inflammation. Clinical findings are not limited to a single mechanism; multiple mechanisms may overlap.
Anti-CTLA-4 inhibitors (ipilimumab) most frequently cause orbital inflammation 2). Similar clinical presentations have been reported with anti-PD-1/PD-L1 inhibitors 2). MRI shows enlargement and contrast enhancement of extraocular muscles and inflammatory changes in orbital fat, with a tendency for bilateral occurrence 2).
7. Latest Research and Future Perspectives (Research-Stage Reports)
With the rapid expansion of ICI indications, the number of cases of ICI-related ocular irAE is expected to increase over the next few decades 1).
Currently, understanding of the pathophysiology of posterior segment irAE is mainly based on case reports and case series, with few experimental studies on mechanisms 1). Diagnostic criteria and treatment guidelines for ICI-associated VKH-like reactions have not been established. While some cases show good treatment response, persistent exudative retinal detachment or ICI-induced occlusive retinal vasculitis can lead to permanent visual impairment 1).
Future challenges include establishing treatment strategies based on the mechanism type of posterior segment irAE, standardizing baseline ophthalmic examinations before ICI administration, and developing collaboration protocols between oncology and ophthalmology.
Haliyur R, Elner SG, Sassalos T, Kodati S, Johnson MW. Pathogenic Mechanisms of Immune Checkpoint Inhibitor (ICI)-Associated Retinal and Choroidal Adverse Reactions. American journal of ophthalmology. 2025;272:8-18. doi:10.1016/j.ajo.2024.12.028. PMID:39755350.
Ang T, Chaggar V, Tong JY, Selva D. Medication-associated orbital inflammation: A systematic review. Surv Ophthalmol. 2024;69(4):622-631. doi:10.1016/j.survophthal.2024.03.003. PMID:38490453.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.