Cosmetic wide conjunctivectomy is a non-therapeutic surgical technique to reduce conjunctival hyperemia for aesthetic purposes. It is commonly called “cosmetic eye whitening.” The bulbar conjunctiva and Tenon’s capsule are resected, and mitomycin C (MMC) is applied to the exposed sclera to inhibit vascular regrowth.
Developed in South Korea in the early 2000s for treating persistent conjunctival hyperemia unresponsive to eye drops. Initial reports indicated high patient satisfaction and low complication rates, leading to rapid adoption across South Korea and parts of Asia. However, a large 2012 study reported that 91.7% of patients experienced at least one postoperative complication. Serious complications such as necrotizing scleritis, which can lead to vision loss, became evident, and the South Korean Ministry of Health and Welfare officially banned this procedure1).
Despite this decision, the procedure was introduced in the United States under the brand name I-BRITE1). Adoption in the US was limited, but similar serious complications as in South Korea have been reported1). Currently, the procedure is rarely performed, but no formal ban exists in the US.
Conjunctival surgery (including eye whitening) can cause iatrogenic dry eye, inflammation, and scarring, potentially damaging the ocular surface2).
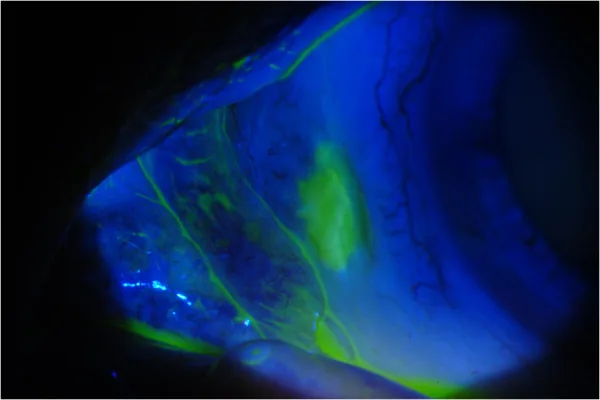
Theresa G Leung, James P Dunn, Esen K Akpek, Jennifer E Thorne Necrotizing scleritis as a complication of cosmetic eye whitening procedure 2013 Feb 22 J Ophthalmic Inflamm Infect. 2013 Feb 22; 3:39 Figure 3. PMCID: PMC3605078. License: CC BY.
Erosion sites on the conjunctiva and sclera stained with fluorescein.
The primary preoperative complaint is cosmetic dissatisfaction due to chronic conjunctival hyperemia. Surgery was considered when the condition was resistant to topical vasoconstrictors, artificial tears, and anti-inflammatory drugs.
Postoperative complications include pain, photophobia, blurred vision, and decreased visual acuity. In the case series by Azar et al., severe pain, photophobia, and blurred vision developed in both eyes 9 years after surgery1).
Postoperative complications are diverse and often appear late, from weeks to years after surgery.
Scleral-related findings:
Scleral thinning: Progressive thinning of the avascular sclera, sometimes with uveal show1)
Calcific plaques: Calcium deposits form on the exposed sclera. In the case by Azar et al., they were noticed as “yellow-white spots” 3 years after surgery1)
Necrotizing scleritis: The most devastating complication. It can occur even in immunocompetent patients, suggesting local ischemia and toxic mechanisms1)
Diplopia: Due to scarring or restricted eye movement
Dry eye: Due to loss of conjunctival goblet cells and ocular surface instability2)
In a retrospective study of 1,713 cases, scleral complications occurred in 186 cases (11%). The breakdown was calcification 6.2%, scleral softening 4.4%, scleritis 0.2%, and scleral necrosis 0.1%1).
Vascular endothelial inhibition: MMC inhibits capillary endothelial cell proliferation in the episcleral vessels, leading to vascular disarray, ischemia, and necrosis1)
Postoperative medication issues: Administering MMC 0.02% four times daily for 2–5 days postoperatively (without irrigation) results in excessive cumulative exposure 1)
Complication risks: High concentrations (0.1%) or prolonged use increase the incidence of scleral melting, corneal melting, iritis, and cataracts 4)
Surgical technique issues
Excessive cauterization: Excessive electrocautery for hemostasis directly damages episcleral vessels, leading to poor wound healing and necrosis 1)
Extensive Tenon’s capsule excision: Tenon’s capsule contributes to ocular surface protection and blood supply; excessive excision increases the risk of ischemia
No wound closure: Many protocols intentionally left the sclera exposed without closure
Other risk factors include contact lens dependence, pre-existing dry eye, history of MMC or radiation exposure, and previous autoimmune scleritis. Cases have been reported where dry eye after LASIK caused chronic hyperemia, prompting eye-whitening surgery 1). Elevated levels of tear mucin-9 and TNF-α after LASIK may contribute to the development of scleral necrosis 1).
MMC is also used to prevent recurrence in pterygium surgery, but it can cause scleral thinning, ulceration, and delayed conjunctival epithelialization 3). In pterygium surgery, intraoperative application of 0.02–0.04% for a short duration (30 seconds to 5 minutes) is standard, which differs greatly from the postoperative daily administration in cosmetic conjunctival resection.
QWhy was this surgery banned in South Korea?
A
A large 2012 study found that 91.7% of patients experienced postoperative complications, revealing severe complications such as necrotizing scleritis that can lead to irreversible vision loss. The fact that it is a cosmetic surgery with no therapeutic necessity also served as grounds for the ban. The Korean Ministry of Health and Welfare issued an order to stop this surgery. In the United States, it was introduced as I-BRITE, but no formal ban has been implemented despite similar complication reports.
Because many complications are delayed, long-term follow-up after surgery is essential. In reported cases, necrotizing scleritis appeared 3 months to 9 years after surgery1).
Ophthalmic evaluation:
Slit-lamp examination: assessment of scleral thinning, presence of uveal show, calcific plaques, and conjunctival epithelial defects
Fluorescein staining: detection of persistent epithelial defects and corneal surface disorders
In the differential diagnosis of necrotizing scleritis, exclusion of autoimmune diseases is necessary. In the case by Azar et al., all autoantibodies except antinuclear antibody (ANA 1:160) were negative, and CRP, ESR, ACE, etc. were also normal1). Similarly, no systemic autoimmune diseases were detected in other reports1). This suggests that the main cause of necrosis is not an autoimmune predisposition but local ischemia due to MMC and cautery.
In the case by Azar et al., treatment was initiated with oral prednisone 60 mg plus topical prednisolone acetate 1% every hour 1). A flare occurred during steroid tapering, and methotrexate 20 mg/week was added, allowing successful steroid taper and discontinuation 1). Complete symptom resolution and recovery of visual acuity to 20/20 were achieved at 3 months after starting treatment 1). Methotrexate was continued for 2 years before tapering and discontinuation, and the patient remained stable without flare at 3 months thereafter 1).
Azar et al. (2023) reported a 36-year-old woman who developed bilateral SISN 9 years after I-BRITE surgery. She had no history of autoimmune disease, and immunological workup revealed no systemic autoimmune disease. Inflammation was controlled with methotrexate, allowing discontinuation of steroids. This is the second report demonstrating the efficacy of immunosuppressive therapy for SISN after cosmetic eye whitening surgery. 1)
Scleral patch graft: management of scleral thinning and perforation risk
Surgical removal of calcified plaques
QCan complications appear many years after surgery?
A
Yes. In reported cases of necrotizing scleritis, it appears late, ranging from 3 months to 9 years after surgery. The longest was in the case of Azar et al., with onset 9 years postoperatively. Because the sclera is a tissue with poor vascularity and slow collagen turnover, ischemia and necrosis progress slowly and may only become clinically apparent after a long period. Therefore, long-term follow-up is essential for patients who have undergone this surgery.
MMC is an alkylating agent cultured from Streptomyces caespitosus 1). It causes DNA damage through two pathways: free radical-mediated DNA and protein damage under aerobic conditions, and DNA alkylation under anaerobic conditions 4). It forms DNA crosslinks between adenine and guanine residues, inhibiting DNA synthesis and arresting cell division 4).
In ophthalmology, it is used to suppress the proliferation of Tenon’s capsule fibroblasts, but it also inhibits capillary endothelial cells of the episcleral vessels 1). This leads to vascular disorganization, ischemia, and necrosis. The sclera is poorly vascularized and relies on the episcleral vessels and choroid for nutrient supply 1). When these vessels are destroyed, the sclera, with its slow collagen turnover, loses its repair capacity.
Excessive electrocautery used for hemostasis during conjunctival resection directly destroys episcleral vessels 1). The inhibition of vascular endothelium by MMC and direct vascular destruction by cautery act additively, leading to irreversible scleral ischemia.
Delayed scleral necrosis may involve a local autoimmune inflammatory reaction 1). Scleral fibroblasts normally express HLA class I molecules, but under inflammatory stimulation, expression of HLA class II molecules (HLA-DR, -DP, -DQ) is induced 1). It is thought that surgical tissue damage causes exposure of self-antigens, triggering a type III hypersensitivity reaction with immune complex deposition in episcleral vessels 1).
This mechanism may explain why SISN occurs even in patients without systemic autoimmune disease and why immunosuppression with methotrexate is effective 1).
Azar et al. (2023) reported the second case of SISN developing 9 years after I-BRITE surgery, treated with methotrexate1). They suggested that the pathology of SISN involves not only local vascular damage but also the generation of local autoimmune inflammation1). Further research into the mechanisms driving this inflammatory response is needed.
Most of the currently available evidence consists of case reports and case series, with no large-scale prospective trials. Because follow-up in cosmetic surgery settings is limited, the true incidence of late complications may be underestimated.
MMC is useful as an adjunctive therapy for pterygium surgery3) and OSSN treatment4), but daily administration for extensive bare sclera exceeds acceptable cumulative toxicity. In pterygium surgery, the standard protocol involves intraoperative application of 0.02% MMC for 30 seconds to 5 minutes followed by irrigation with saline3), which is fundamentally different from the cosmetic conjunctival resection protocol.
Available evidence indicates that cosmetic extensive conjunctival resection carries an unacceptably high risk of delayed, irreversible complications. No consistently safe modification of the surgical technique has been demonstrated.
Azar NS, Ruiz-Lozano RE, Quiroga-Garza ME, Soifer M, Mousa HM, Komai S, et al. Delayed presentation of surgically induced scleral necrosis after I-BRITE procedure treated with immunosuppressive therapy. Digital journal of ophthalmology : DJO. 2023;29(3):77-82. doi:10.5693/djo.02.2023.04.005. PMID:37780039; PMCID:PMC10539002.
Wolffsohn JS, Arita R, Chalmers R, et al. TFOS DEWS II iatrogenic report. Ocul Surf. 2023.
Chu WK, Choi HL, Bhat AK, Jhanji V. Pterygium: new insights. Eye (London, England). 2020;34(6):1047-1050. doi:10.1038/s41433-020-0786-3. PMID:32029918; PMCID:PMC7413326.
Tsatsos M, Delimitrou C, Tsinopoulos I, Ziakas N. Update in the Diagnosis and Management of Ocular Surface Squamous Neoplasia (OSSN). J Clin Med. 2025;14(5):1699. doi:10.3390/jcm14051699.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.