Multiple endocrine neoplasia (MEN) is a rare group of hereditary disorders with an increased risk of developing neoplasms in two or more endocrine glands. It follows an autosomal dominant inheritance pattern with high penetrance and variable expressivity.
Prevalence: 1 in 35,000 people (for all MEN type 2)
Ophthalmic features: Marked corneal nerve thickening, conjunctival and eyelid neuromas (especially in MEN type 2B)
The ophthalmic features of MEN are classically described in MEN type 2B. In MEN type 2B, in addition to medullary thyroid carcinoma and pheochromocytoma, mucosal neuromas and intestinal ganglioneuromatosis occur. Mucosal neuromas are found in nearly 100% of patients with MEN type 2B and are known as a pathognomonic finding of this syndrome. Ophthalmic findings may provide clues for early diagnosis of MEN type 2B 5).
In MEN type 1, a large cohort from the Dutch MEN1 Study (323 cases) showed that 38.1% of patients developed pituitary tumors 3). Prolactinoma is the most common pituitary tumor and responds well to drug therapy with dopamine agonists.
QAt what age are ophthalmic findings of MEN type 2B recognized?
A
The characteristic findings of MEN type 2B can be recognized from childhood. Corneal nerve thickening and mucosal neuromas appear early and may be the first clinical clues of MEN type 2B. MTC in MEN type 2B can develop in infancy, and early recognition of ophthalmic findings influences the timing of diagnosis and preventive treatment.
Prominent corneal nerves are the most characteristic ocular finding in MEN2B. Thickened nerve fibers in the cornea are observed by slit-lamp microscopy. Histopathologically, they are unmyelinated nerves with Schwann cells, and the axons appear normal. In MEN2A, according to Kinoshita et al., grade 2 or higher corneal nerve thickening was observed in 16 of 28 eyes (57%), and marked thickening of grade 3–4 was observed in about 29%, making it an important ocular finding in MEN in general 1).
Conjunctival and eyelid neuromas are recognized as thickened nerve proliferations without a capsule. Similar mucosal neuromas also appear on the lips, tongue, and buccal mucosa. In vivo confocal microscopy (IVCM) shows irregular arrangement of large, thick nerve bundles, loops, branching, and dilatation up to 1 mm in conjunctival neuromas, and thickening of the subbasal nerve plexus in the cornea6). In pediatric cases, mucosal neuromas around the limbus have been reported to cause secondary open-angle glaucoma requiring intraocular pressure management 2).
In MEN1, the main ophthalmic problem is chiasmal syndrome due to pituitary tumors. Bitemporal hemianopia with a vertical meridian boundary is most frequently observed on visual field testing. Optic atrophy may also be present.
Non-ophthalmic features (MEN2B) include lip hypertrophy, Marfanoid habitus, and intestinal ganglioneuromatosis (which can cause megacolon).
QIf the corneal nerves appear thickened, should MEN always be suspected?
A
Prominent corneal nerves are not specific to MEN2B. They are also seen in Refsum syndrome, Hansen disease, Riley-Day syndrome, neurofibromatosis, and congenital ichthyosis. Additionally, corneal nerves may be prominent in corneal diseases such as keratoconus, herpes simplex keratitis, and posterior polymorphous corneal dystrophy. However, they are usually not as prominent as in MEN2B. Diagnosis is made in combination with other systemic findings (lip hypertrophy, Marfanoid habitus, etc.).
MEN syndromes follow an autosomal dominant inheritance pattern. Individuals with RET mutations have a 50% risk of passing the mutation to offspring. Sporadic cases due to somatic mutations also exist.
Mutations in the MEN1 gene (chromosome 11q13) are the cause. The MEN1 gene encodes a protein called menin, a tumor suppressor. Loss of function occurs via a “two-hit” mechanism with mutations in both alleles, leading to uncontrolled cell proliferation.
Missense mutations in the RET proto-oncogene (chromosome 10q11.2) are the cause. The RET protein is a tyrosine kinase receptor involved in the differentiation and migration of neuroendocrine tissues. Mutations result in gain-of-function abnormalities, leading to tumor development.
In MEN2B, approximately 95% of patients have a germline mutation at codon 918 (M918T mutation) 4). Patients with this mutation develop the disease in infancy and present with the most aggressive form of MTC. On the other hand, diagnosis of MEN2B patients tends to be delayed; in a Japanese case series by Nagaoka et al., all four patients had mucosal neuromas and gastrointestinal symptoms from infancy, yet were first diagnosed at the stage of symptomatic MTC 5).
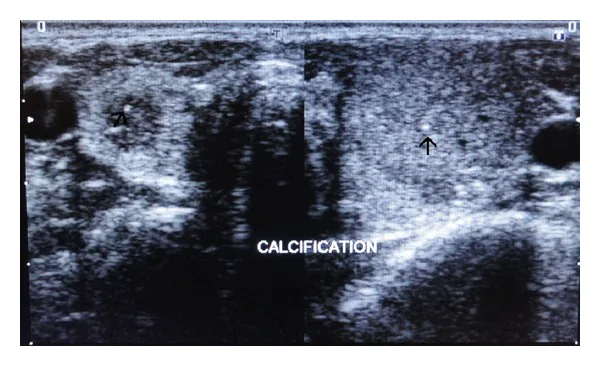
Mehtab Ahmad, Imran Rizvi, Amit Jain, Noorin Zaidi Painful Hip Leading to the Diagnosis of MEN 2B Syndrome 2012 Nov 26 Case Rep Endocrinol. 2012 Nov 26; 2012:567060 Figure 2. PMCID: PMC3513729. License: CC BY.
Ultrasound images of the left and right thyroid show punctate hyperechoic calcifications within the parenchyma, indicated by arrows. This is an evaluation image of thyroid lesions that are problematic in multiple endocrine neoplasia.
The diagnosis of MEN syndromes is usually based on family history and non-ophthalmic findings. Ophthalmic examination is particularly useful for detailed evaluation in new cases.
Slit-lamp microscopy: Essential for observing corneal nerve thickening and conjunctival/eyelid neuromas
In vivo confocal microscopy (IVCM): Non-invasively visualizes characteristic large nerve bundles and loop structures of conjunctival neuromas, as well as thickening of the corneal subbasal nerve plexus 6)
Goldmann perimetry (GVF): Used to evaluate chiasmal syndrome due to pituitary tumors in MEN1. Bitemporal hemianopia is the most frequent finding.
Ishihara color vision test: Used to evaluate color vision impairment due to pituitary tumors
High-resolution optical coherence tomography (HR-OCT): Used for non-invasive evaluation of conjunctival neuromas and useful for differentiation from other diseases
Multidisciplinary collaboration is essential for the management of MEN patients. Clinical geneticists, endocrinologists, surgeons, and oncologists are involved.
Genetic counseling should be performed prior to RET genetic testing. In families with MEN2, screening should be performed at birth or as early as possible. Genetic counseling should be offered to all first-degree relatives of newly diagnosed probands with RET mutations.
For patients with germline mutations at codons 883, 918, or 922 in MEN2B, total thyroidectomy and central lymph node dissection should be performed within the first few months of life, because the lifetime penetrance of MTC is nearly 100%.
Ophthalmologists play a key role in early detection of ocular manifestations in MEN, appropriate referral, and visual rehabilitation. For pituitary tumors in MEN1, regular visual field testing and visual acuity assessment are necessary. In MEN2B, management of dry eye and regular intraocular pressure measurement are performed.
QWhat ophthalmic follow-up is necessary when diagnosed with MEN2B?
A
In MEN2B, regular slit-lamp examination is performed to observe changes in corneal nerves and conjunctival/palpebral neuromas. Dry eye symptoms should be assessed and managed with artificial tears as needed. Due to the risk of open-angle glaucoma, regular intraocular pressure measurement and visual field testing are also recommended. In addition, imaging studies should be performed to evaluate for the presence of pituitary tumors.
MEN1 develops due to loss of function of a tumor suppressor gene based on the “two-hit hypothesis.” The first mutation (germline mutation) is inherited, and the second mutation (somatic mutation) is acquired later, leading to complete loss of menin protein function and loss of control of cell proliferation.
Menin is expressed in both endocrine and non-endocrine tissues, but the exact mechanism leading to carcinogenesis remains unclear. Pituitary tumors compressing the optic chiasm cause bitemporal hemianopsia.
RET protein is a tyrosine kinase receptor involved in the differentiation and migration of developing neuroendocrine tissues. Missense mutations in the RET gene result in a single amino acid substitution, causing constitutive activation (gain of function) of the protein.
RET is expressed in multiple tissues including thyroid parafollicular cells (C cells), parathyroid glands, intestinal ganglia, adrenal chromaffin cells, and peripheral and central nervous systems. This broad expression pattern explains the diverse tumor patterns in MEN2.
Histopathological examination of thickened corneal nerves in MEN2B shows unmyelinated nerves with Schwann cells. Axons have a normal appearance and vary in diameter from 0.1 to 1.4 nm. Conjunctival and eyelid neuromas appear as non-encapsulated nerve proliferations.
Kinoshita S, Tanaka F, Ohashi Y, Ikeda M, Takai S. Incidence of prominent corneal nerves in multiple endocrine neoplasia type 2A. American journal of ophthalmology. 1991;111(3):307-11. doi:10.1016/s0002-9394(14)72314-1. PMID:1672053.
Chang TC, Okafor KC, Cavuoto KM, Dubovy SR, Karp CL. Pediatric Multiple Endocrine Neoplasia Type 2B: Clinicopathological Correlation of Perilimbal Mucosal Neuromas and Treatment of Secondary Open-Angle Glaucoma. Ocular oncology and pathology. 2018;4(3):196-198. doi:10.1159/000484053. PMID:29765955; PMCID:PMC5939668.
de Laat JM, Dekkers OM, Pieterman CRC, Kluijfhout WP, Hermus AR, Pereira AM, et al. Long-Term Natural Course of Pituitary Tumors in Patients With MEN1: Results From the DutchMEN1 Study Group (DMSG). J Clin Endocrinol Metab. 2015;100(9):3288-3296. doi:10.1210/jc.2015-2015.
Wells SA, Asa SL, Dralle H, Elisei R, Evans DB, Gagel RF, Lee N, Machens A, Moley JF, Pacini F, Raue F, Frank-Raue K, Robinson B, Rosenthal MS, Santoro M, Schlumberger M, Shah M, Waguespack SG, American Thyroid Association Guidelines Task Force on Medullary Thyroid Carcinoma. Revised American Thyroid Association guidelines for the management of medullary thyroid carcinoma. Thyroid. 2015;25(6):567-610. doi:10.1089/thy.2014.0335. PMID:25810047; PMCID:PMC4490627.
Nagaoka R, Sugitani I, Sanada M, Jikuzono T, Okamura R, Igarashi T, et al. The Reality of Multiple Endocrine Neoplasia Type 2B Diagnosis: Awareness of Unique Physical Appearance Is Important. Journal of Nippon Medical School = Nippon Ika Daigaku zasshi. 2018;85(3):178-182. doi:10.1272/jnms.JNMS.2018_85-26. PMID:30135345.
Lam D, Villaret J, Nguyen Kim P, Gabison E, Cochereau I, Doan S. In Vivo Confocal Microscopy of Prominent Conjunctival and Corneal Nerves in Multiple Endocrine Neoplasia Type 2B. Cornea. 2019;38(11):1453-1455. doi:10.1097/ICO.0000000000002028. PMID:31205161.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.