Focal choroidal excavation (FCE) is a localized concave change in the choroid detected by optical coherence tomography (OCT). It is characterized by the absence of posterior staphyloma or scleral ectasia. It was first reported by Jampol in 2006 and named by Margolis et al. in 2011.
FCE morphology is broadly classified into two types.
Conforming type
Definition: A type in which there is no separation between the photoreceptor outer segment and the RPE (retinal pigment epithelium).
Features: The photoreceptors and RPE remain attached and sink together within the excavation. It often follows a relatively stable course.
OCT findings: The RPE and photoreceptor layer in the concavity are displaced together toward the choroid.
Non-conforming type
Definition: A type in which a gap (subretinal fluid or hyperreflective material) is observed between the photoreceptor outer segments and the RPE.
Features: High risk of complications such as macular neovascularization (choroidal neovascularization) and serous retinal detachment.
OCT findings: Fluid accumulation or hyperreflective material is observed between the RPE and photoreceptor layer within the concavity.
Classification by shape (conical, bowl-shaped, mixed) and by location (foveal, extrafoveal) is also used.
Capellan et al. classified FCE into three types based on etiology: type 1 (myopic), type 2 (congenital), and type 3 (acquired/inflammatory). In type 3, the rate of CNV (choroidal neovascularization) reaches 40% 7).
The prevalence in individuals under 40 years is reported to be 0.18% (3 out of 1697 eyes) 1). The prevalence of FCE in patients with central serous chorioretinopathy (CSC) is 2.8–7.8%, higher than in the general population 1). Detection rates are increasing with the widespread use of OCT.
In recent years, FCE has been trending toward exclusion from the pachychoroid disease spectrum. It is now considered an independent condition resulting from inflammatory Bruch’s membrane defects and localized choroidal thinning 8).
QIs focal choroidal excavation (FCE) a rare disease?
A
The prevalence in individuals under 40 years is low at 0.18%, but incidental detection is increasing with the widespread use of OCT1). Many cases are asymptomatic and are first noticed during fundus examination or OCT.
Many cases are asymptomatic and discovered incidentally during OCT examination. Symptomatic cases present the following.
Metamorphopsia: Straight lines appear distorted. A report of metamorphopsia with best-corrected visual acuity (BCVA) of 20/40 in a 30-year-old woman exists2).
Central scotoma: A dark area in the central visual field.
FFA (fluorescein fundus angiography): Late hyperfluorescence (leakage or staining only) is observed1)5). In extrafoveal FCE, late staining without edema is characteristic5).
OCT: Shows localized choroidal excavation that is diagnostic. It can differentiate between conforming and non-conforming types.
OCTA: Shows dark flow signals (void areas) in the choriocapillaris layer of the FCE area 1). When macular neovascularization is present, flower-like net-shaped new vessels are visualized 2).
QIs treatment necessary even if there are no symptoms?
A
If there are no symptoms and no macular neovascularization or serous retinal detachment, observation is the basic approach. However, due to the risk of developing macular neovascularization, regular monitoring with OCT and OCTA is recommended (see “Standard Treatment” section for details).
The pathogenesis of FCE has not been fully elucidated, and several hypotheses have been proposed.
Congenital developmental disorder hypothesis: It is thought to be formed congenitally due to abnormal choroidal development during the embryonic period3).
Acquired Bruch’s membrane defect hypothesis: Outer layer tissue protrudes outward due to intraocular pressure at sites of Bruch’s membrane degradation or defects, leading to FCE formation4). A characteristic feature is that the internal limiting membrane is not displaced.
Inflammation hypothesis (latest hypothesis): This theory proposes that inflammation causes Bruch’s membrane defects and localized choroidal thinning, resulting in FCE formation8). Based on this hypothesis, FCE is considered a condition independent of the pachychoroid spectrum.
Direct evidence related to ABCA4: In Stargardt disease (ABCA4-associated retinopathy), small Bruch’s membrane defects precede FCE formation, which was confirmed by continuous OCT observation over 8 years7).
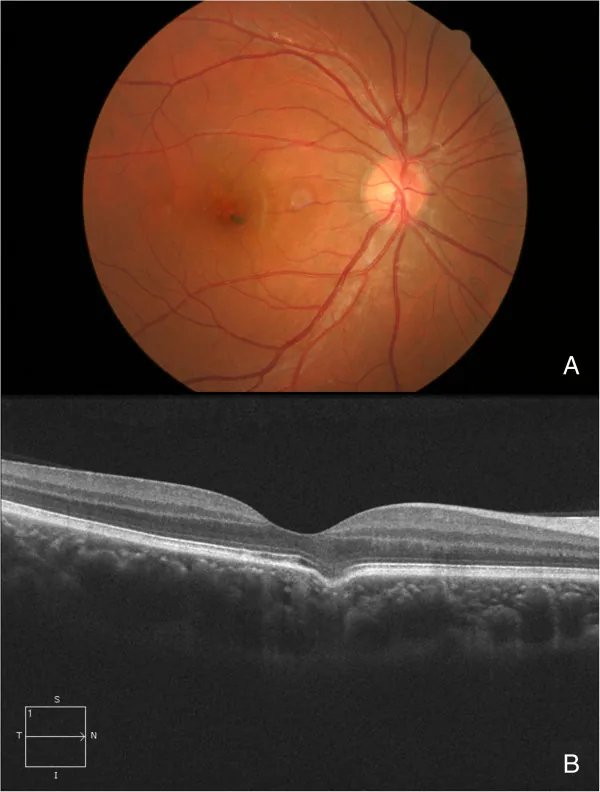
Jie Guo; Lu Zhong; Chunhui Jiang; Xin Zhou; Gezhi Xu; Wenji Wang; Yuliang Wang. Clinical and optic coherence tomography findings of focal choroidal excavation in Chinese patients. BMC Ophthalmol. 2014 May 6; 14:63. Figure 3. PMCID: PMC4107723. License: CC BY.
Fundus image and OCT of an eye with a solitary excavation. These images are from a 30-year-old male who underwent a routine general exam. (A) There were some pigmentary changes at the macula. (B) An excavation at the fovea was present on the OCT.
OCT is essential for diagnosing FCE. Diagnosis and evaluation are performed using a combination of the following tests.
OCT
Role: Gold standard for diagnosis.
Findings: Focal choroidal excavation. It is possible to distinguish between conforming and non-conforming types. Shape (cone, bowl, mixed) and depth are also measured.
OCTA
Role: Non-invasive detection of macular neovascularization. Diagnosis is possible without contrast agent2).
Findings: Dark flow signal void area in the choriocapillaris layer of the FCE region. When complicated by macular neovascularization, a flower-like net of neovascularization is depicted 2).
FA and ICGA
FA findings: Late hyperfluorescence (leakage/staining). Useful for evaluating CNV and RPE degeneration5).
ICGA findings: Evaluation of choroidal vascular structure. Useful for assessing pachychoroid and dilated choroidal vessels4).
Other auxiliary tests may include FAF (evaluation of RPE health) and B-mode ultrasound (to differentiate from posterior staphyloma).
For asymptomatic cases without choroidal neovascularization or serous retinal detachment, regular follow-up is the basic policy. Lifelong OCT and OCTA monitoring is recommended 1).
In a bilateral case of FCE complicated with CSC, a combination of focal laser (spot size 50 μm, power 70 mW, duration 0.1 seconds) and SML (Subthreshold Micropulse Laser) resulted in resolution of serous retinal detachment after 5 months 1).
Anti-VEGF therapy for cases with choroidal neovascularization
Anti-VEGF therapy is the first-line treatment for cases with choroidal neovascularization. The main treatment outcomes are shown below.
Study
Drug
Outcome
Duke 20252)
Bevacizumab 1.25mg/0.05mL
20/40 to 20/20 after 3 injections
Sato 20214)
Aflibercept monthly × 3 months
CNV resolution + FCE resolution, no recurrence at 12 months
Literature summary4)
Anti-VEGF overall
54 of 76 eyes (71%) showed good anatomical response
Duke RCT et al. (2025) reported a case of a 30-year-old woman with subfoveal choroidal neovascularization (CNV) associated with FCE who received three injections of Bevacizumab, resulting in regression of the flower-like net-shaped CNV on OCTA and improvement in BCVA from 20/40 to 20/202).
Sato et al. (2021) reported a case in which monthly Aflibercept injections for three months led to the disappearance of CNV and the FCE itself4). No recurrence of CNV or FCE was observed during 12 months of follow-up. The disappearance of FCE is presumed to be due to fibrovascular scar formation after anti-VEGF therapy bridging the Bruch’s membrane defect.
Focal laser photocoagulation: Considered for localized exudation outside the fovea.
Cryotherapy: Occasionally used as an adjunct for peripheral lesions.
QIf choroidal neovascularization occurs, can it be cured with treatment?
A
Anti-VEGF therapy is effective, with good anatomical response reported in 54 of 76 eyes (71%) 4). In some cases, the FCE itself may disappear 4). However, due to the risk of recurrence, continuous monitoring after treatment is necessary.
6. Pathophysiology and Detailed Mechanism of Onset
The most widely supported theory is the Bruch membrane defect hypothesis. At sites of Bruch membrane weakening or defect, the outer layer of the RPE-Bruch membrane complex protrudes outward due to intraocular pressure (IOP). The internal limiting membrane (ILM) does not shift. This matches the morphological features of FCE observed on OCT4).
OCTA analysis reveals dark flow signal void areas in the choriocapillaris layer of the FCE region1). This suggests reduced blood flow in the choriocapillaris at the FCE site, and local ischemia may lead to inflammation, Bruch’s membrane fragility, and macular neovascularization2).
The following pathway is estimated: choroidal depression → localized choroidal thinning → ischemia/chronic inflammation → Bruch’s membrane weakening → macular neovascularization2). In type 3 FCE, the rate of CNV complication has been reported to reach 40% 7), making the classification of FCE types important for clinical risk assessment.
Alagille syndrome (AGS) is a multi-organ disease caused by JAG1 gene mutations (over 97%). Against a background of chorioretinal atrophy due to abnormal Notch signaling pathway, FCE and macular hole have been reported to co-occur 6).
7. Latest research and future perspectives (reports at research stage)
Conventionally, FCE was sometimes included in the pachychoroid disease spectrum, but recent large-scale reviews have led to reclassification. Cheung et al. (2024) proposed excluding FCE from the pachychoroid disease spectrum and positioning it as an independent pathology with inflammatory Bruch’s membrane defects and localized choroidal thinning as the etiology 8).
Eight-year observation in ABCA4-associated retinopathy
Benson et al. followed FCE in ABCA4-associated retinopathy with serial OCT over eight years and documented for the first time the natural course of conforming FCE transitioning to non-conforming FCE and eventually leading to macular hole7). This observation is an important finding for understanding the progression of FCE.
Non-invasive diagnosis of macular neovascularization using OCTA+SD-OCT
It has been reported that combining OCTA (optical coherence tomography angiography) and SD-OCT (spectral-domain OCT) enables diagnosis of FCE-associated macular neovascularization without the use of contrast agents (fluorescein, ICGA)2). This may reduce dependence on invasive contrast examinations.
Sato et al. (2021) reported the first case of FCE itself disappearing after Aflibercept administration4). Bridging of Bruch’s membrane defects by fibrovascular scar is speculated as the mechanism of FCE disappearance, suggesting that anti-VEGF therapy may also affect morphological changes in FCE.
The three-type classification by Capellan et al. (type 1: myopic, type 2: congenital, type 3: acquired/inflammatory) is attracting attention as a useful framework for risk assessment and treatment decision-making7). Validation through future prospective large-scale studies is expected.
QWill FCE worsen in the future?
A
Most FCEs follow a stable course, but the rate of macular neovascularization is reported to be approximately 16% in long-term follow-up 2). In cases with underlying progressive retinal degeneration such as ABCA4-related retinopathy, there are reports of gradual deepening from the conforming type to the non-conforming type, leading to macular hole7). Lifelong monitoring is recommended 1).
Bai J, Wang Y, Cao N, Liu Y, Chen X, He T, et al. Bilateral Focal Choroidal Excavation and Central Serous Chorioretinopathy Coexisting in a Male Patient. Case reports in ophthalmological medicine. 2024;2024:5519361. doi:10.1155/2024/5519361. PMID:38566845; PMCID:PMC10987251.
Duke RCT, Anshumali S, Crosson JN. Optical Coherence Tomography Angiography in Macular Neovascularization Secondary to Focal Choroidal Excavation. Journal of vitreoretinal diseases. 2025;9(2):228-231. doi:10.1177/24741264241294159. PMID:39539837; PMCID:PMC11556386.
Belenje A, Takkar B, Narayanan R, Jalali S. Unilateral focal choroidal excavation in cone dystrophy. BMJ Case Rep. 2021;14:e240665. doi:10.1136/bcr-2020-240665. PMID:33541964; PMCID:PMC7868241.
Sato T, Yasukawa T, Hayashi K. Focal choroidal excavation disappearing after successful treatment of type 2 choroidal neovascularization with intravitreal aflibercept. American journal of ophthalmology case reports. 2021;22:101078. doi:10.1016/j.ajoc.2021.101078. PMID:33869893; PMCID:PMC8044643.
Dhodapkar RM, Spadaro JZ, Adelman RA. A case of extrafoveal focal choroidal excavation. American journal of ophthalmology case reports. 2022;27:101682. doi:10.1016/j.ajoc.2022.101682. PMID:35990800; PMCID:PMC9385540.
Misawa M, Tampo H, Makino S.. Atypical Focal Choroidal Excavation with Macular Hole in a Patient with Alagille Syndrome. Case Rep Ophthalmol Med. 2022;2022:8136115. doi:10.1155/2022/8136115. PMID:36105151; PMCID:PMC9467701.
Benson MD, Feldman CB, Zein WM. Evolution of focal choroidal excavation in ABCA4-related retinopathy. American journal of ophthalmology case reports. 2022;28:101740. doi:10.1016/j.ajoc.2022.101740. PMID:36393906; PMCID:PMC9647336.
Cheung CMG, Lai TYY, Ruamviboonsuk P, et al. Pachychoroid disease. Eye. 2024;38:797-808.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.