Definition
OCT diagnostic criteria: inward protrusion of 50 μm or more from the tangent line to the outer surface of the RPE at the base of posterior staphyloma
First report: first described by Gaucher et al. in 2008

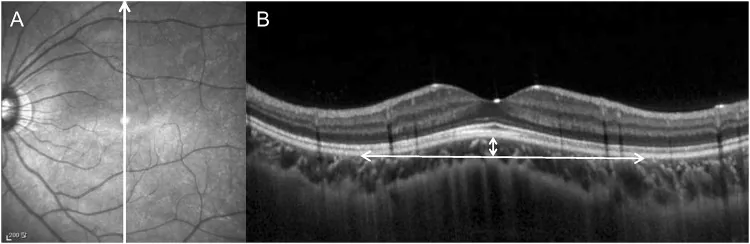
Dome-shaped macula (DSM) is a morphological abnormality in which the macula protrudes anteriorly (toward the vitreous) relative to the posterior ocular wall, occurring in the context of high myopia and posterior staphyloma (concave deformation within the staphyloma). It was first reported by Gaucher et al. in 2008 1).
On OCT (optical coherence tomography) images, it is defined as a macular elevation protruding more than 50 μm inward from the tangent line to the outer surface of the RPE (retinal pigment epithelium) at the floor of the posterior staphyloma 1). The prevalence in hospital-based high myopia eyes is reported to be 10.7–12% 1).
Unilateral DSM can also occur in hyperopic or emmetropic eyes, and reports exist in mild myopia or non-myopic eyes.
Definition
OCT diagnostic criteria: inward protrusion of 50 μm or more from the tangent line to the outer surface of the RPE at the base of posterior staphyloma
First report: first described by Gaucher et al. in 2008
Prevalence
High myopia (hospital-based): 10.7–12%
Occurrence in non-myopic eyes: unilateral DSM has also been reported in hyperopic and emmetropic eyes
Morphological diversity
Horizontal oval: Most common (62%)
Central round: 21%
Vertical oval: 17%
DSM is classified into three morphological types.
| Type | Features | Frequency |
|---|---|---|
| Horizontal oval dome | Widely covers the macula horizontally | 62% (most common) |
| Central round dome | Elevation concentrated in the central macula | 21% |
| Vertical oval dome | Vertically elongated shape | 17% |
The main OCT findings are as follows.
Fluorescein angiography (FA) may show pinpoint leakage, and indocyanine green angiography (ICGA) may show localized punctate hyperfluorescence.
Takahashi et al. (2023) reported a case of ridge-shaped DSM in both eyes of an 84-year-old woman (right eye axial length 27.41 mm, left eye 28.17 mm). In the right eye, the sclera split into inner and outer layers with only the inner layer protruding forward, while in the left eye, uniform thickening of the foveal sclera was observed1).
If there are no complications, it often remains asymptomatic. DSM without SRF or CNV is often discovered incidentally on OCT examination, and visual acuity is relatively preserved. Regardless of the presence or absence of symptoms, regular ophthalmologic examinations are important for individuals with high myopia.
High myopia (severe nearsightedness) is the greatest risk factor, and elongation of the axial length (26.5 mm or more) causes stretching of the posterior wall and formation of posterior staphyloma 2). Advanced age is also considered a related factor.
The exact etiology of DSM has not been elucidated. The following mechanisms have been proposed.
The main etiological hypotheses are shown below.
| Hypothesis | Proponent/Evidence |
|---|---|
| Localized thickening of the subfoveal sclera | Imamura et al., observation by EDI-OCT |
| Scleral splitting due to intrascleral vessels | Takahashi et al. (2023) 1) |
| Reduced scleral tension due to Bruch’s membrane defect | Takahashi et al. (2023) 1) |
| Localized thickening of the choroid | Multiple observational studies |
| Posterior wall collapse and vitreomacular traction | Inferred from morphological features |
Intrascleral vessels (short posterior ciliary arteries, long posterior ciliary arteries, and branches of the macular vortex vein) may be involved in the formation and morphology of DSM1). It has also been discussed that DSM may play a protective role in preventing traction damage to the fovea due to long axial length.
OCT is an essential test for diagnosing DSM. Radial scanning is recommended, and obtaining cross-sections in both vertical and horizontal directions improves the accuracy of morphological evaluation.
The main examination and diagnostic methods are as follows:
The following diseases should be considered in the differential diagnosis.
| Differential diagnosis | Key points for differentiation |
|---|---|
| Central serous chorioretinopathy (CSC) | Presence of posterior staphyloma, macular morphology |
| Choroidal hemangioma, amelanotic melanoma | Characteristics of elevated lesion, ultrasound findings |
| Bilateral diffuse uveal melanocytic proliferation (BDUMP) | Systemic evaluation / bilateral |
| Uveal effusion syndrome | Associated peripheral exudative retinal detachment |
| Posterior scleritis | Pain / inflammatory signs / ultrasound |
There is currently no established effective treatment. The main goals of management are reduction of SRF (serous subretinal fluid) and maintenance of visual acuity.
Observation
Indications: Asymptomatic cases, small amount of SRF, good visual acuity.
Course: SRF often recurs after resolution, requiring regular OCT follow-up.
Anti-VEGF Therapy
Aflibercept: Monthly injections for 3 months have been reported to improve BCVA and reduce central foveal thickness.
Bevacizumab and Ranibizumab: Studies have shown no significant improvement in BCVA or complete resolution of SRF.
When CNV is present: Intravitreal ranibizumab is used 1)
Other Treatments
Photodynamic therapy: Efficacy results are mixed and not established.
MRA (mineralocorticoid receptor antagonist): Limited reports of resolution of serous foveal detachment.
Vitrectomy: Temporary resolution of subretinal detachment has been reported, but it is not standard.
A study of 56 eyes reported that none of bevacizumab, ranibizumab, or photodynamic therapy achieved significant improvement in BCVA or complete resolution of SRF.
Currently, there is no established treatment. For mild, asymptomatic cases without SRF, observation is the basic approach. Aflibercept is attracting attention as a promising option, but evidence is still limited. If CNV is present, anti-VEGF treatment is essential.
The main mechanism of DSM formation is proposed to be localized thickening of the subfoveal sclera (based on Imamura et al.’s EDI-OCT study)1). However, why this thickening occurs remains unknown1).
In a 2023 report by Takahashi et al., a unique morphology was observed in which the sclera is divided into inner and outer layers by intrascleral blood vessels, with only the inner layer protruding forward while the outer layer remains in a normal position 1). The involved vessels are the short posterior ciliary arteries (SPCAs), long posterior ciliary arteries (LPCAs), and branches of the macular vortex veins, and around the cross-sections of these vessels, scleral fibers are pushed outward and deformed into a rhomboid shape 1).
Furthermore, it has been suggested that Bruch’s membrane defects around the macula may locally reduce scleral tension and contribute to the formation of DSM 1). Perforating vessels are frequently observed around CNV (myopic choroidal neovascularization) and may be involved in the development of CNV 1).
The following mechanisms are considered for the development of SRF:
It has also been hypothesized that the DSM plays a protective role by preventing traction damage to the fovea and distributing traction forces to the periphery.
Axial elongation causes the posterior ocular wall to stretch anteroposteriorly, leading to the formation of posterior staphyloma. During this process, localized thickening of the foveal sclera occurs, which is thought to result in the formation of DSM. Bruch’s membrane defects causing reduced scleral tension and scleral splitting due to intrascleral vessels may also be involved 1).
Carlà et al. (2025) reported in a 15-year follow-up study of a European cohort that 37% of 220 eyes with DSM developed myopic maculopathy (MNM) (OR 4.95, 95% CI 3.50-6.97, P<0.0001) 2). In eyes without DSM, the incidence of MNM was only 11%.
The same study showed that DSM and lacquer cracks were significantly correlated with neovascular complications 2). On the other hand, DSM itself was not correlated with worse visual prognosis after MNM onset 2). Myopic maculopathy progressed over more than 10 years in 57% of cases, and active myopic CNV (N2a stage) developed in 190 eyes (15%), confirmed after an average of 4.5±1.8 years 2).
Takahashi et al. (2023) first reported in detail the unique morphology of the sclera splitting into two layers in DSM using swept-source OCT and EDI-OCT 1). It was suggested that blood vessels running within the sclera are involved in the splitting, drawing attention to the role of scleral vessels in DSM formation.
Research on the long-term prognosis of DSM suggests the following as important prognostic factors.
BCVA often remains stable for several years, but long-term reports indicate that 37% develop MNM, which is a higher risk compared to eyes without DSM (11%) 2). A dome height exceeding 400 μm is a poor prognostic factor. Regular ophthalmologic follow-up is important.