Choroidal osteoma is a benign osseous choristoma in which mature bone tissue forms in the choroid. It is characterized by replacement of the choroidal stroma with mature bone.
It was first reported at the 1975 Verhoeff Society meeting. A 26-year-old woman with a paracentral scotoma presented with a yellowish-white subretinal tumor on the nasal side of the optic disc in the left eye. It commonly occurs in the posterior pole of young women in their 10s to 30s. It is usually unilateral, but about 20% of cases are bilateral.
It is a rare tumor, with only 61 cases reported over 26 years at a tertiary medical center. Significant vision loss can occur in about 60% of affected eyes. 1) It has also been reported that up to 90% of ophthalmologists miss it on initial examination. 1)
Fundus findings are characterized by a well-defined, map-like, yellowish-white to orange, flat lesion located in the posterior pole. Over time, pigmentation, RPE atrophy, and decalcification occur, changing the fundus appearance. The lesion gradually enlarges but eventually stops.
QCan choroidal osteoma become malignant?
A
Malignant transformation has not been reported; it is essentially a benign tumor. However, secondary choroidal neovascularization can significantly reduce vision. For details, see the section on “Standard Treatment”.
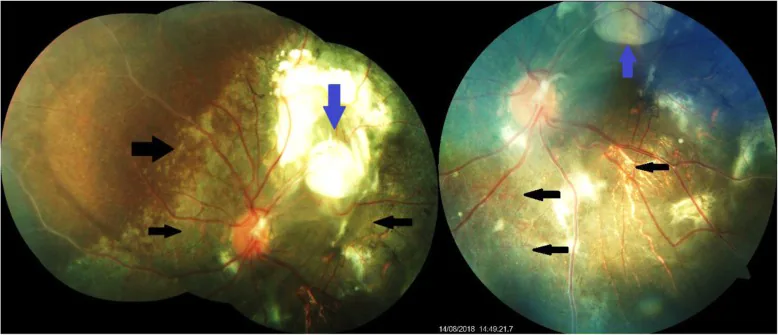
Arup Deuri; Deepanjan Ghosh; Jayant Ekka; Vijaya Agarwalla. Multiple choroidal osteomas in a boy – a rare presentation: a case report. J Med Case Rep. 2019 Aug 2; 13:238 Figure 1. PMCID: PMC6676636. License: CC BY.
Fundus photograph of the left eye showing multiple choroidal osteomas superotemporally (blue arrows) and areas of retinal pigment epithelium depigmentation (black arrows)
The following findings are observed in the posterior pole of the fundus, especially around the optic disc.
Yellow-white to yellow-orange patchy lesions: Flat lesions with well-defined geographic borders. There is almost no elevation, and fine vessels are often present on the tumor surface.
Brown, orange, or gray pigment clumping: Irregular pigmentation on the tumor surface.
Depigmentation: Thin, atrophic yellowish-gray areas with RPE atrophy. Seen in advanced cases or after treatment.
Degeneration and atrophy of RPE and outer retina: The RPE and photoreceptors degenerate and atrophy as the disease progresses.
The cause of choroidal osteoma is unknown. Several hypotheses have been proposed regarding why ectopic bone formation occurs in the choroid, but no definitive factor has been identified.
Proposed contributing factors are listed below.
Inflammation/trauma: A theory that local inflammation or trauma induces ectopic ossification.
Hormonal status: Since it is more common in young women, involvement of sex hormone secretion is suspected.
Calcium metabolism abnormality: Investigated due to similarity to ectopic calcification, but no consistent correlation with serum Ca, P, or ALP has been found.
Genetic/environmental factors: Involvement is suggested, but no definitive genetic pattern has been identified.
Choristoma hypothesis: The theory that bone tissue, which normally does not exist, becomes misplaced during development.
QIs choroidal osteoma hereditary?
A
Genetic factors are suggested to be involved, but a definitive inheritance pattern has not been identified. Although there are reports of family history, it is not established as a hereditary disease.
High-reflectivity lines are observed within the choroid. 1) It is also useful for evaluating photoreceptor atrophy, choroidal compression, and subretinal fluid. OCT angiography (OCTA) is useful for detecting choroidal neovascularization.
A high-attenuation area equivalent to bone is depicted corresponding to the tumor. This is the most specific test leading to a definitive diagnosis and is useful for differentiating from other choroidal masses.
Additionally, differentiation from sclerochoroidal calcification and amelanotic melanoma is necessary. Acoustic shadowing on B-mode ultrasound and bone density confirmation on CT are decisive for differentiation. 1)
Diagnosis is often possible by combining clinical findings with ultrasound and OCT. CT is useful for definitive diagnosis by showing high absorption areas similar to bone, but it is not mandatory in all cases. It is particularly helpful in difficult-to-diagnose cases or when differentiation from other choroidal tumors is needed.
Plan: Continue regular follow-up with fundus examination, OCT, and visual acuity measurement.
Note: If you experience changes in vision, metamorphopsia, or blurred vision, you should see a doctor promptly. Early detection of new choroidal neovascularization is important.
Treatment for Choroidal Neovascularization
Intravitreal anti-VEGF injection: Bevacizumab and ranibizumab are used. 1) This aims to resolve subretinal fluid and hemorrhage associated with choroidal neovascularization.
Photodynamic therapy (PDT): A spot size of 6,000 μm is standard; multiple sessions may be given for large tumors. It minimizes retinal damage while also expecting tumor regression.
The protocol based on the TAP study is used as a reference. A spot size of 6,000 μm is standard, and multiple sessions may be performed for large tumors. PDT allows treatment of the lesion while minimizing damage to the surrounding retina, and is expected to induce regression of the tumor itself. In Japan, PDT for choroidal osteoma is an off-label treatment.
If bullous retinal detachment occurs over the tumor, vitrectomy with subretinal fluid drainage and intraoperative laser photocoagulation may be performed.
QIs it okay not to treat?
A
For asymptomatic and stable lesions, observation is the basic policy. However, if choroidal neovascularization occurs, vision loss may progress rapidly, requiring prompt treatment intervention. It is important to continue regular ophthalmologic examinations and watch for the appearance of new symptoms.
Choroidal osteoma is classified as a congenital osseous choristoma. It is characterized histologically by the replacement of choroidal stroma with mature bone.
Histologically, mature bone tissue is observed. The marrow spaces are filled with loose connective tissue and dilated thin-walled vessels. The marrow vessels communicate with the sub-Bruch’s membrane capillary network and degenerated RPE.
Tumors commonly occur adjacent to or around the optic disc and can extend to the macula. The lesion gradually expands peripherally but tends to eventually stop.
Decalcification occurs naturally but can also happen after laser photocoagulation or PDT. It is observed on the fundus as a thinned, atrophic yellowish-gray area of the tumor. At the advancing edge of decalcification, tumor enlargement tends to stop, which may be associated with scar stabilization of the tumor.
7. Latest Research and Future Perspectives (Investigational Reports)
The average tumor growth rate is reported to be approximately 0.37 mm per year. Long-term poor vision is associated with subretinal fluid, RPE changes, and subretinal hemorrhage from choroidal neovascularization. Progression of decalcification is also a predictor of poor vision.
For extrafoveal calcified osteomas, a strategy has been proposed to prevent tumor enlargement by decalcifying the tumor margin using PDT. This is based on the observation that tumor growth does not occur in areas where decalcification has progressed. However, prospective studies to prove the effectiveness of this treatment strategy are still limited.
Misdiagnosis Patterns and Diagnostic Accuracy Improvement
In a report of two atypical cases by Machado et al. (2024), choroidal osteoma was misdiagnosed as age-related macular degeneration and choroidal hemangioma. 1) In one case, an irregular lesion in the posterior pole was treated as age-related macular degeneration, and in the other, an orange-red fundus finding was misdiagnosed as hemangioma. Acoustic shadowing on B-mode ultrasound and identification of high-reflective lines within the choroid on OCT are key to improving diagnostic accuracy.
Based on reports that up to 90% of ophthalmologists miss the diagnosis at the initial visit 1), the importance of including this disease in the differential diagnosis for posterior pole lesions in young women is being reaffirmed. The widespread use of multimodal imaging is expected to contribute to improved diagnostic accuracy.